


Why Weight Loss Works Differently for Indians — The Metabolic Context First
Understanding this section makes every tip that follows 3x more effective — because it explains the specific mechanisms driving Indian weight gain that most advice completely misses.
TOFI (Thin Outside, Fat Inside): South Asians have a genetic predisposition to store fat as visceral fat (around internal organs) rather than subcutaneous fat, even at low or normal BMI. A person with BMI 22 may have the metabolic risk of a Western person with BMI 28. Standard weight loss advice focused on BMI underestimates Indian metabolic risk and overestimates the safety of being “not overweight.”
Insulin resistance at lower BMI: Indians develop insulin resistance at lower body weights than Western populations. Insulin resistance means cells respond less to insulin → more insulin is needed → insulin stays elevated → fat storage is activated more aggressively. The primary driver: the Indian dietary staple pattern of white rice + maida produces the repeated large insulin spikes that drive insulin resistance faster in genetically predisposed South Asian populations.
The waist circumference standard for Indians: The appropriate metabolic risk threshold for Indian adults is men above 90cm waist circumference and women above 80cm — lower than Western standards (102/88cm) — because visceral fat accumulates at lower overall body fat in South Asians. Waist circumference is a more meaningful health metric than BMI for Indians. Measure your waist at the narrowest point between ribs and hip, not at the belt line.
The good news: Because the primary driver is a specific dietary pattern (high-glycaemic carbohydrates + insufficient protein + late dinners) rather than purely genetic inevitability, targeted dietary changes produce significantly faster metabolic improvement in South Asians than the same changes in Western populations. The body is more responsive to intervention precisely because the intervention targets the highest-leverage driver.

10 Weight Loss Tips That Actually Work for Indians
The most powerful single dietary change for Indian weight loss is not eating less — it is changing what you eat your carbohydrates as. White rice and maida (refined wheat) have high glycaemic indices (73 and 70+ respectively) that produce large, rapid insulin spikes after eating. Every insulin spike activates fat storage, and repeated daily insulin spikes from 3 meals of white rice/maida progressively drive insulin resistance — the metabolic state that makes fat loss increasingly difficult. Millets — ragi (finger millet), bajra (pearl millet), jowar (sorghum), and foxtail millet — have lower glycaemic indices, significantly higher fibre, higher protein, and dramatically higher micronutrient density (particularly magnesium, which improves insulin sensitivity).
A 2021 systematic review and meta-analysis in Frontiers in Nutrition found that replacing refined cereals with millets significantly reduced fasting blood glucose, HbA1c, postprandial glucose, and body weight — with effects comparable to standard diabetes management. The weight loss mechanism: lower postprandial insulin → less fat storage signalling, higher fibre → greater satiety hormone (GLP-1, PYY) release → lower food intake at the next meal, and the improved insulin sensitivity from magnesium → cells respond better to existing insulin → less compensatory insulin production required.
⚗️ Frontiers in Nutrition 2021 meta-analysis: millets significantly reduced glucose + HbA1c + body weight vs refined cereals | Ragi: 137mg Mg/100g vs white rice 12mg | 3x fibre
Protein is the most powerful macronutrient for weight loss — more so than any other dietary change. It has three simultaneous weight loss mechanisms: thermogenesis (your body burns 20–30% of protein calories just to digest it, compared to 5–10% for carbohydrates and 0–3% for fat), appetite regulation (protein reduces ghrelin — the hunger hormone — and increases GLP-1, PYY, and CCK — the satiety hormones — more powerfully than any other macronutrient), and muscle preservation during a caloric deficit (maintaining muscle preserves resting metabolic rate — every kg of muscle burns 13–20 extra calories daily at rest).
The India-specific problem: most Indian urban diets provide approximately 40–50g of protein daily — significantly below the 72–90g target for a 60kg person wanting to lose weight. The typical Indian breakfast (poha, upma, idli without sambar, plain paratha) is almost entirely carbohydrate. The lunch dal is protein-containing but rarely in therapeutic quantities. The dinner sabzi and roti is again carbohydrate-dominant. Building protein into every eating occasion — not just the main meal — is the practical intervention.
⚗️ Protein thermogenesis: 20–30% caloric cost vs 5–10% carbs | Ghrelin suppression + GLP-1/PYY increase = hunger reduction | Each 1kg muscle = 13–20 extra kcal/day resting metabolism
This is the weight loss strategy with the best benefit-to-effort ratio available: changing the order in which you eat your existing food — without restricting any food or counting any calorie. A landmark 2015 Weill Cornell study found that eating vegetables and protein before carbohydrates reduced the postprandial blood glucose spike by 40–50% and the insulin response proportionally — from the identical meal, simply reordered. The mechanism: protein and fibre in the stomach before carbohydrates arrive slows gastric emptying rate (food moves from stomach to small intestine more slowly), viscous fibre forms a gel that slows glucose absorption, and protein triggers GIP and GLP-1 release that moderates the insulin response before the carbohydrate glucose load arrives.
For weight loss: lower insulin spikes → less fat storage signalling → over months, significantly less visceral fat accumulation. For blood sugar: 40–50% lower postprandial glucose from the same meal — one of the most clinically significant dietary interventions for diabetes prevention and management available without any food restriction. This costs nothing, changes nothing about the food itself, and takes zero willpower. For more detail: Lower Blood Sugar Naturally
⚗️ Weill Cornell 2015: meal sequencing = -40–50% postprandial glucose spike | Same food, different order | Viscous fibre + protein slows gastric emptying → insulin moderation
Post-meal walking is the most underrated and most accessible weight loss intervention available — and the science behind it is more compelling than most people know. When muscles contract during walking, GLUT4 transporters are activated independently of insulin — they translocate to the cell membrane and allow glucose to enter muscle cells without insulin signalling. Walking after a meal intercepts the postprandial glucose peak at its highest point, removing glucose from the bloodstream through the most insulin-efficient mechanism available. A 2022 Sports Medicine meta-analysis found that three 10-minute post-meal walks reduced the 24-hour glucose area under the curve more effectively than a single 30-minute walk done at any time of day — not just for blood sugar, but for insulin, triglycerides, and the downstream fat storage signals.
For weight loss specifically: consistent post-meal walking improves systemic insulin sensitivity over weeks, reduces the insulin-driven visceral fat deposition that is the primary mechanism of Indian belly fat, builds the daily movement habit that is more metabolically significant than occasional intense exercise, and activates fat oxidation pathways that continue for 1–2 hours after the walk. The ancient Indian practice of shatapawali (a walk of 100 steps after meals) is physiologically precise — this is its modern validation. For the belly fat connection: How to Lose Belly Fat Naturally
⚗️ 2022 Sports Medicine meta-analysis: post-meal walks outperform single daily walk for 24h glucose | GLUT4 activation: insulin-independent glucose uptake | 3 × 10 min > 1 × 30 min
Liquid calories are the most commonly overlooked source of caloric surplus in Indian diets — and the most easily reduced without affecting satisfaction. The Indian chai habit: 3–4 cups of chai daily with 2 tsp sugar each = 24–32 tsp sugar = 96–128g sugar = 384–512 calories from sugar alone — before any food is counted. Add cold drinks (a 300ml can of cola = 33g sugar = 132 calories), commercial fruit juice (a glass = 25–30g sugar = 100–120 calories), flavoured lassi or packaged curd drinks, and sweetened milk — the typical urban Indian can easily consume 600–800 calories daily from beverages alone while feeling like they have not eaten anything.
Liquid calories are particularly weight-promoting because they do not trigger the satiety hormones that solid food does — the stomach’s stretch receptors that signal fullness are not activated by liquids, and the chewing process that initiates hormonal satiety signalling does not occur. A 500-calorie cola produces no satiety; a 500-calorie meal produces significant satiety. Reducing liquid sugar is therefore the most calorie-efficient weight loss intervention per unit of subjective deprivation — the sacrifice is relatively small, the caloric reduction is large.
⚗️ Liquid calories: no gastric stretch receptor activation = no satiety = not compensated by eating less | 4 daily chai + 1 cold drink = 600–800 extra calories with zero hunger reduction
The timing of when you eat matters almost as much as what you eat — because insulin sensitivity follows a circadian rhythm that is highest in the morning and lowest in the evening. The same quantity of carbohydrates consumed at 8am produces a 20–30% lower insulin response than at 8pm. Evening carbohydrates consumed when insulin sensitivity is lowest are the most likely to be stored as fat rather than burned for energy. The Indian cultural norm of making dinner the largest meal of the day — often eaten at 9–10pm in urban households after a long day — is the dietary pattern most aligned with fat storage and least aligned with fat loss.
A 2020 Cell Metabolism RCT found that time-restricted eating aligned with circadian rhythms (eating window ending by 6–7pm) significantly reduced visceral fat, blood pressure, and cholesterol without any dietary restriction. A 2013 randomised trial found that eating the same total calories — with the majority at breakfast rather than dinner — produced 2.5x greater weight loss over 12 weeks. For Indians practically: move dinner earlier (ideally before 8pm), make it the lightest meal of the day (dal-sabzi without additional rice if possible, or a smaller rice portion), and stop all eating 2–3 hours before sleep.
⚗️ Circadian insulin sensitivity: highest morning, lowest evening | Cell Metabolism 2020: early TRE → visceral fat reduction | 2013 RCT: morning-heavy calories = 2.5x greater weight loss vs dinner-heavy
No dietary strategy overcomes the hormonal effects of chronic sleep deprivation. A 2010 Annals of Internal Medicine study found that sleep restriction (5.5 hours vs 8.5 hours) on identical caloric intake produced significantly more fat gain and specifically more visceral fat. The mechanisms: poor sleep raises ghrelin (hunger hormone) by 24%, reduces leptin (satiety hormone) by 18%, increases cortisol (promotes visceral fat storage), impairs insulin sensitivity (reducing glucose disposal in muscle), increases cravings for high-sugar high-fat foods the following day, and reduces the motivation and energy for physical activity.
India averages 6.6 hours of sleep nationally — well below the 7–8 hours associated with optimal metabolic health. The urban professional population averages even less. The weight loss consequence: chronically sleep-deprived individuals consistently lose less fat and more muscle from the same dietary intervention compared to well-rested individuals. Sleep is not a lifestyle luxury to optimise after diet and exercise are perfect — it is a foundational metabolic prerequisite. For comprehensive sleep strategies: Home Remedies for Better Sleep and Why You Wake Up Between 2am–4am
⚗️ Annals Internal Medicine 2010: same calories + less sleep = significantly more fat gained | Ghrelin +24% (hunger up) | Leptin -18% (satiety down) | Cortisol elevation → visceral fat preference
Visceral fat cells have approximately 4 times the glucocorticoid (cortisol) receptor density of subcutaneous fat cells — meaning visceral fat is disproportionately sensitive to cortisol’s fat-storage signals. When cortisol is chronically elevated from work stress, financial pressure, relationship tension, or poor sleep, it specifically directs fat deposition to the visceral depot — the belly, love handles, and upper back — while simultaneously mobilising peripheral fat (arms and legs). This produces the characteristic combination of belly fat with relatively lean limbs seen in chronically stressed urban Indians. An 80% India stress prevalence combined with this mechanism is a major contributor to India’s visceral fat epidemic.
Stress management is not a soft complement to “real” weight loss interventions — it is a direct mechanism intervention for the most metabolically dangerous form of fat. A 2012 Obesity journal study found that 8-week mindfulness-based stress reduction significantly reduced abdominal fat and cortisol. Ashwagandha (documented -27.9% serum cortisol in 2012 RCT) is the most evidence-backed natural cortisol-reduction intervention — and has a direct belly fat reduction mechanism through this cortisol pathway. For the complete cortisol guide: How to Reduce Cortisol Naturally
⚗️ Visceral fat: 4x glucocorticoid receptor density | Cortisol → preferential visceral fat storage | 2012 MBSR RCT: significant abdominal fat + cortisol reduction | Ashwagandha 2012 RCT: -27.9% serum cortisol
Cardio burns calories during exercise. Resistance training changes the metabolic rate at which your body operates 24 hours a day. Every kilogram of muscle tissue added increases resting metabolic rate by 13–20 calories per day — modest individually, but compounding significantly with each kg of muscle. More importantly: resistance training produces a 24–48 hour elevation in insulin sensitivity post-exercise — each session extends fat-mobilising capacity far beyond the workout itself. The 2013 Obesity Reviews meta-analysis confirmed resistance training significantly reduced visceral fat in overweight adults, independently of aerobic exercise. Indian adults have significantly lower skeletal muscle mass relative to fat mass compared to age-matched Western populations — this “low muscle-to-fat” ratio is a major contributor to metabolic risk and makes adding muscle through resistance training particularly impactful for Indian body composition.
No gym is required. Bodyweight resistance training — squats, lunges, push-ups, planks, glute bridges, resistance band rows — 3 sessions of 30 minutes weekly produces meaningful muscle mass increase and metabolic improvement within 8–12 weeks. The most important principle: progressive overload — gradually making exercises harder over time (more reps, more sets, or more weight) is what maintains the muscle-building signal. An unchanging routine stops producing stimulus within 4–6 weeks.
⚗️ 1 kg muscle = 13–20 extra kcal/day resting metabolic rate | 48-hour post-exercise insulin sensitisation | Obesity Reviews 2013: RT reduces visceral fat independently | Low muscle mass = primary Indian metabolic risk
The Indian spice cabinet is not flavouring — it is a pharmacy. Several common Indian spices have documented mechanisms directly relevant to weight management: Jeera (cumin) — a 2014 RCT found 3g cumin daily for 3 months produced significant waist circumference and body fat reduction, with improved fasting glucose and insulin. Dalchini (cinnamon) — cinnamaldehyde activates AMPK (AMP-activated protein kinase), the same enzyme pathway as metformin (first-line diabetes drug), improving insulin sensitivity. Methi (fenugreek) — 4-hydroxyisoleucine is a natural insulin secretagogue that stimulates insulin only when glucose is present, preventing postprandial glucose spikes without hypoglycaemia. Haldi (turmeric) — curcumin inhibits adipogenesis (fat cell formation) and reduces visceral fat inflammatory signalling. Kali mirch (black pepper) — piperine inhibits the formation of new fat cells and improves the bioavailability of all other active spice compounds by up to 2,000%.
These are not magic weight loss supplements at the concentrations used in cooking — they are metabolic adjuncts that, consistently present in daily cooking, shift insulin sensitivity, reduce postprandial glucose, and reduce fat cell signalling across months and years of regular consumption. The traditional Indian spice-heavy cooking tradition was inadvertently metabolic medicine — and the shift toward plain, spice-reduced modern cooking has removed this daily metabolic support. For more: Best Morning Drinks for Gut Health & Fat Loss
⚗️ Jeera 2014 RCT: significant waist + fat reduction | Cinnamon cinnamaldehyde: AMPK = metformin mechanism | Methi 4-hydroxyisoleucine: glucose-dependent insulin secretion | Turmeric: adipogenesis inhibition
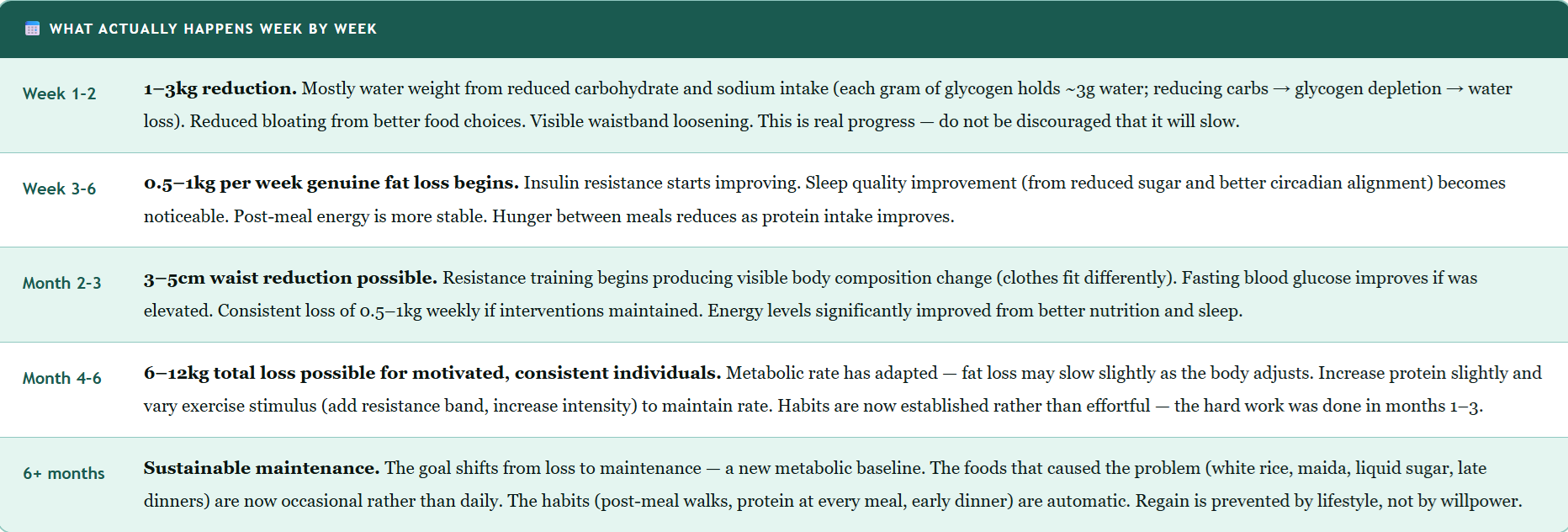
A Realistic Weight Loss Timeline — What to Expect and When

What Doesn’t Work — Save Your Money and Your Willpower
Severe calorie restriction (crash diets, starvation, detox cleanses): Produces rapid initial weight loss (mostly water and muscle), then triggers starvation adaptation — metabolic rate drops, cortisol spikes (increasing visceral fat storage), muscle is catabolised (reducing resting metabolic rate), and the inevitable rebound regains all weight as fat. The second attempt is harder than the first because the metabolic rate has been suppressed and lean muscle mass reduced.
“Fat-free” and “sugar-free” products: Fat-free products replace fat with sugar and refined starch (both insulin-spiking). Sugar-free products use artificial sweeteners (sorbitol, aspartame) that maintain sweet taste expectations, disrupt gut microbiome, and may paradoxically worsen insulin response. Real whole food is metabolically superior to processed “diet” food.
Juice detox fasts for weight loss: Eliminate dietary protein (required for muscle preservation) and provide high fructose loads (driving liver fat accumulation). Any weight lost is water and muscle — not fat. See: Full Body Detox: What Actually Works
Weight loss supplements without evidence: Garcinia cambogia, raspberry ketones, green coffee extract — have no meaningful clinical evidence for fat loss at commercial doses. The money is better invested in whole food quality.
Exercise without dietary change: Exercise alone produces modest weight loss (approximately 1–2kg over 3 months without dietary change). Exercise is essential for muscle building, insulin sensitivity, and metabolic health — but the dietary change produces the caloric deficit that drives fat loss. Both are required for optimal results.
Indian Weight Loss Myths vs. Facts
“Indian food is inherently fattening and I need to eat Western food to lose weight.”
Traditional whole-food Indian cooking — dal, sabzi, ragi, bajra, curd, fish, seasonal vegetables, spiced with turmeric and jeera — is among the most metabolically supportive diets in the world. What is fattening is the modern Indian diet — refined versions of Indian food (maida paratha, white rice, sweetened chai, namkeen, packaged food). The solution is returning to traditional whole-food Indian cooking, not abandoning Indian food.
“Ghee and coconut oil are fattening and should be completely avoided.”
1–2 tsp ghee daily in home cooking is not the cause of Indian weight gain — the large quantities of refined carbohydrates and sugar are. Ghee provides butyrate (gut health), CLA (anti-adipogenic), and fat-soluble vitamins that support hormonal function. The problem is restaurant cooking where 3–5 tbsp ghee per dish significantly elevates caloric content. Home cooking with controlled amounts of ghee is appropriate for weight loss.
“Vegetarians cannot lose weight effectively because they can’t get enough protein.”
Vegetarians can absolutely achieve adequate protein for weight loss — but it requires intentionality. The combination of dal + rice or dal + roti provides complete amino acids through protein complementarity. Adding paneer, curd, eggs (for ovo-vegetarians), sattu, rajma, and chana to every meal provides 80–100g protein daily. The common Indian mistake: calling dal + rice a “complete meal” when the protein content is 8–10g rather than the 20–25g target per eating occasion.
Frequently Asked Questions
The fastest legitimate weight loss for Indians comes from addressing the highest-leverage drivers simultaneously: (1) Switch grains — ragi/bajra/jowar replacing white rice and maida immediately reduces daily insulin load and glycaemic variability, the primary drivers of Indian visceral fat. (2) Eliminate liquid sugar — 3–4 cups of sweetened chai daily may represent 400–500 hidden calories; switching to plain chai or herbal tea produces the fastest visible reduction. (3) Post-meal walking — 10–15 minutes after each meal activates GLUT4 (insulin-independent glucose disposal), directly reducing fat storage signals. (4) Early light dinner — before 8pm; exploiting the circadian insulin advantage. Combined, these four changes — without any calorie counting — typically produce 1–2kg loss in the first two weeks and 0.5–1kg per week thereafter.
Realistic fat loss: 2–4 kg per month (0.5–1 kg per week). The first week often shows 2–4kg due to water weight loss from glycogen depletion — this is real but not all fat. Sustainable fat-only loss is approximately 0.5 kg per week. Faster rates (above 1 kg fat per week) typically involve significant muscle loss, metabolic adaptation, hormonal disruption, and rebound weight gain. For long-term maintenance: people who lose 0.5–1 kg per week are 3x more likely to maintain the loss at 5 years than those who lose aggressively.
The best Indian weight loss diet: whole grains replacing refined (ragi, bajra, whole wheat instead of white rice and maida), protein at every meal (dal + paneer/curd/eggs — targeting 1.2–1.5g per kg body weight), vegetables-before-carbs meal sequencing (-40–50% insulin spike from same meal), no liquid sugar, early light dinner before 8pm, generous traditional spices (turmeric, jeera, methi, cinnamon), and adequate water. No special diet required — traditional whole-food Indian cooking is the answer. The problem was never Indian food; it was the modern refined version of it.
Yes — a 12-hour eating window (breakfast by 8am, finish dinner by 8pm) is sustainable, culturally compatible, and produces meaningful metabolic benefit. The 16:8 protocol is more aggressive and effective but challenging if late family dinners are the norm. Critical adaptation for India: do NOT skip breakfast during the eating window — skipping breakfast causes blood sugar drop → cortisol spike → visceral fat deposition. Indian IF = early breakfast + substantive lunch + light early dinner, not breakfast-skipping. People with diabetes on insulin or sulphonylureas: consult endocrinologist before starting.
The TOFI (Thin Outside, Fat Inside) phenomenon — South Asians genetically store fat as visceral fat preferentially, at lower BMI than Western populations. Combined with: higher insulin resistance prevalence (even in lean Indians), a dietary pattern of high-glycaemic carbohydrates that maximally activate the fat-storing insulin pathway these bodies are most sensitive to, and increasingly sedentary lifestyles. The intervention: targeting insulin resistance through grain quality, protein, and meal timing — not simply eating less. Reducing refined carbohydrates and increasing protein produces faster and more significant results in Indians than in populations without this genetic pattern, precisely because the intervention targets the highest-leverage driver.
Related Articles You’ll Love
Losing weight in India is not about eating less. It is about understanding the specific metabolic machinery of the Indian body — the visceral fat genetics, the insulin sensitivity that responds so powerfully to carbohydrate quality, the circadian insulin advantage that makes morning eating physiologically superior to evening eating, and the stress-cortisol-belly fat cycle that no treadmill session can outrun.
Swap the grains. Add the protein. Walk after every meal. Move dinner earlier. Sleep better. Manage the stress. Use the spices that your kitchen has carried for generations. These are not 10 abstract tips. They are 10 interventions in the specific mechanisms that drive Indian weight gain. Target the mechanism. The weight follows.
Start today: eat vegetables before rice at your next meal. Walk for 10 minutes after it. The biology will do the rest — over time. 🌿Which tip surprised you most — the meal sequencing 40–50% glucose reduction, the post-meal walk outperforming a gym session, or the circadian insulin advantage that makes dinner the worst time for carbohydrates? Share this with every Indian family navigating weight management — the mechanisms make all the difference. 👇
Sources & Further Reading
- Frontiers in Nutrition (2021) — Millets vs Refined Cereals Meta-analysis: Significantly Reduced Glucose, HbA1c, and Body Weight
- Diabetes Care (2015) — Meal Sequencing: Eating Vegetables Before Carbohydrates Reduces Postprandial Glucose by 40–50%
- Sports Medicine (2022) — Post-Meal Walks Meta-analysis: Three 10-min Walks Outperform Single 30-min Walk for 24h Glucose
- Annals of Internal Medicine (2010) — Sleep Restriction and Fat Gain: Same Calories + Less Sleep = More Visceral Fat
- Obesity (2013) — Calorie Timing RCT: Morning-Heavy vs Evening-Heavy Distribution — 2.5x Greater Weight Loss
- Complementary Therapies in Clinical Practice (2014) — Cumin (Jeera) RCT: Significant Waist Circumference and Body Fat Reduction
- Obesity (2012) — Mindfulness-Based Stress Reduction and Abdominal Fat: Significant Reduction Through Cortisol Normalisation
- HerbeeLife — How to Lose Belly Fat Naturally: The TOFI + Insulin Science Guide
- HerbeeLife — Natural Health & Ayurvedic Wellness
Disclaimer: This content is for informational and educational purposes only. People with diabetes, PCOS, thyroid conditions, or other metabolic conditions should consult a qualified dietitian and physician before making significant dietary changes. Weight loss interventions should be individualised. Read full disclaimer →