The India Paradox — Why a Sunny Country Has a Vitamin D Crisis
Indoor lifestyles: Most urban Indian professionals spend 8–12 hours daily in offices, then commute in vehicles and return home after dark. Total direct outdoor sun exposure is often under 15 minutes. Vitamin D synthesis requires direct UVB exposure — not ambient daylight.
Glass blocks UVB entirely: Sitting beside a sunny window is warming and pleasant but produces zero Vitamin D. Glass transmits UVA (which causes skin tanning and ageing) but blocks UVB (280–315nm) — the specific wavelength required to convert 7-dehydrocholesterol in skin to previtamin D3.
High melanin requires much more sun: Melanin — the pigment that gives Indian skin its colour — competes with 7-dehydrocholesterol for UVB photons in the skin. Darker skin requires 3–6x longer sun exposure than fair skin to produce equivalent Vitamin D. A 10-minute guideline from a European study applied to Indians is biologically incorrect.
Air pollution blocks UVB: India’s major cities have heavy particulate matter pollution that significantly attenuates UVB reaching the ground — even in summer. Outdoor workers in Delhi, Mumbai, and Chennai may receive substantially less UVB per hour than their counterparts in rural areas with clear skies, despite being in a sunnier climate.
Vegetarian diet has no D3: Vitamin D3 is found almost exclusively in animal products — fatty fish, egg yolks, liver. India’s predominantly vegetarian population has no adequate dietary source of D3. The widely claimed “plant sources” of Vitamin D are D2 (ergocalciferol) from mushrooms — which is significantly less effective than D3 at raising serum 25-OH Vitamin D levels.
Magnesium deficiency blocks activation: Even when Vitamin D is present, it cannot become biologically active without magnesium. Two sequential hydroxylation steps — in the liver and kidneys — require magnesium-dependent enzymes. Most Indians are simultaneously deficient in both nutrients, making supplementation of D3 alone insufficient. See: What Magnesium Deficiency Does to Your Body
Understanding Your 25-OH Vitamin D Level — What the Numbers Mean
The correct test for Vitamin D status is 25-OH Vitamin D (25-hydroxyvitamin D / calcidiol) — the storage form. Not “1,25-dihydroxyvitamin D” (the active form, which is tightly regulated and stays in the normal range even with severe deficiency). Request 25-OH Vitamin D specifically.

The Self-Assessment — Check Every Symptom That Applies to You
These symptoms — consistent for 4+ weeks without another identified cause — are associated with Vitamin D deficiency. Checking 5 or more strongly suggests testing is warranted.
Persistent fatigue — tired even after adequate sleep, low energy through the day
Deep bone aching — shins, back, ribs, hips — described as “pain in the bone”
Muscle weakness — difficulty climbing stairs, rising from chair, lifting arms overhead
Frequent illness — repeated colds, slow healing, infections that linger
Low mood or depression — persistent low mood, particularly in winter months
Hair loss or thinning — diffuse hair fall, related to VDR signalling in follicles
Poor sleep quality — difficulty falling asleep or staying asleep
Sweating of the head — excessive head sweating, particularly in infants and adults at night
Slow wound healing — cuts and injuries take unusually long to heal
Back pain — lower back pain unrelated to injury or posture
Frequent headaches or migraines — recurrent without clear trigger
Brain fog or poor concentration — cognitive difficulties, word-finding problems
12 Signs of Vitamin D Deficiency — The Biology Behind Each
Vitamin D receptors (VDRs) are expressed in skeletal muscle fibres — Vitamin D directly regulates calcium handling within muscle cells, muscle protein synthesis, and mitochondrial function. Deficiency produces a characteristic, deep, diffuse aching in muscles and bones — particularly the shins, lower back, ribs, and hips. It is often described as “pain inside the bone” rather than on the surface — reflecting the underlying bone tissue involvement (osteomalacia — softening of the bone matrix from inadequate calcium mineralisation). The pain is typically worse after rest and in the morning, improving slightly with movement. Proximal muscle weakness is the other cardinal physical sign — difficulty performing activities that require strong proximal muscles: climbing stairs, rising from a seated position without using the arms, reaching overhead. This is one of the most commonly misattributed symptom clusters in India — blamed on arthritis, fibromyalgia, or old age, when a 25-OH Vitamin D test and correction would resolve it. For more: Why Your Body Aches All the Time
⚗️ VDRs in skeletal muscle: regulate Ca²⁺ handling + protein synthesis | Bone matrix calcium mineralisation failure = osteomalacia | Morning-worse = classic musculoskeletal Vitamin D pattern
The fatigue of Vitamin D deficiency is not ordinary tiredness from insufficient sleep — it is a cellular-level energy failure. VDRs are expressed in mitochondrial membranes and regulate the expression of enzymes involved in oxidative phosphorylation (the cellular process that produces ATP — the body’s energy currency). When Vitamin D is deficient, mitochondrial function is suboptimal — cells produce less ATP per unit of substrate, producing the characteristic feeling of fatigue that is not relieved by sleep. A 2015 study confirmed that correcting Vitamin D deficiency significantly reduced fatigue scores in deficient individuals. The India-specific burden: most chronically fatigued Indians are tested for anaemia and thyroid dysfunction but not Vitamin D — yet Vitamin D deficiency affects 3–4 times more people than clinical hypothyroidism in India.
⚗️ VDRs in mitochondrial membrane → oxidative phosphorylation regulation | ATP deficiency = cellular fatigue | 2015: correcting deficiency significantly reduced fatigue scores
VDRs are expressed in every major immune cell type: T cells, B cells, macrophages, dendritic cells, and natural killer cells. Vitamin D regulates the production of cathelicidin and defensins — antimicrobial peptides that are the innate immune system’s first-line defence against bacteria and viruses. It also modulates the adaptive immune response, suppressing excessive inflammatory responses while enhancing pathogen-targeted immunity. Multiple meta-analyses confirm that Vitamin D supplementation significantly reduces the risk of acute respiratory infections — with a 2017 BMJ meta-analysis of 25 trials (11,321 participants) finding that supplementation reduced the risk of respiratory infection by 12% overall and by 50% in severely deficient individuals. The seasonal pattern of respiratory illnesses in India — peaking in the monsoon months when sun exposure is lowest and population Vitamin D levels have dropped further — is partly a Vitamin D story.
⚗️ VDRs in all immune cells | Cathelicidin + defensin production → first-line antimicrobial defence | 2017 BMJ meta-analysis (11,321 participants): -12% respiratory infection risk; -50% in severely deficient
VDRs are expressed throughout the brain — in the hippocampus, cingulate cortex, thalamus, and substantia nigra. Vitamin D regulates the expression of tryptophan hydroxylase (the enzyme that converts tryptophan to serotonin — the “mood molecule”), tyrosine hydroxylase (dopamine synthesis), and p11 (a protein involved in serotonin receptor function). Deficiency reduces serotonin production and increases neuroinflammatory signalling — both mechanisms implicated in depression. Multiple observational studies show significant associations between low Vitamin D and depression; a 2020 meta-analysis of randomised controlled trials found Vitamin D supplementation significantly improved depression scores, particularly in individuals who were deficient at baseline. The pattern in India: low mood and fatigue that worsens during the monsoon and winter months (lower sun exposure → lower Vitamin D) without any identifiable life event cause is a strong signal for Vitamin D deficiency.
⚗️ VDRs in brain regulate tryptophan hydroxylase (serotonin) + tyrosine hydroxylase (dopamine) | 2020 meta-analysis: supplementation significantly improved depression scores in deficient individuals
Hair follicles express VDRs — Vitamin D signalling through these receptors is directly involved in regulating the hair follicle cycle. VDR knockout mice develop alopecia (hair loss) without developing rickets — demonstrating that the hair follicle effect of Vitamin D is independent of its bone calcium effects. In humans, multiple studies confirm significantly lower Vitamin D levels in women with hair loss compared to age-matched controls. A 2013 study specifically found lower Vitamin D in women with both telogen effluvium (diffuse shedding) and female pattern hair loss. The mechanism: VDR signalling promotes the transition from telogen (resting) back to anagen (active growth) — deficiency prolongs the resting phase and shortens the growth phase, producing progressive thinning. For the complete hair loss picture: Why Your Hair Is Falling Out Suddenly
⚗️ VDRs in dermal papilla cells regulate anagen ↔ telogen cycling | VDR knockout → alopecia without rickets | 2013: significantly lower Vitamin D in women with telogen effluvium and FPHL
Vitamin D receptors are present in the brain regions that regulate circadian rhythms and sleep — including the suprachiasmatic nucleus (the master circadian clock) and the pineal gland (melatonin production centre). Vitamin D influences the expression of circadian clock genes (CLOCK, BMAL1, Per1) that determine the timing and quality of sleep architecture. A 2018 study found that Vitamin D deficiency was significantly associated with poor sleep quality, short sleep duration, and impaired sleep efficiency. A 2017 randomised trial found that correcting Vitamin D deficiency in deficient individuals significantly improved sleep quality and duration. The mechanism includes Vitamin D’s regulation of serotonin (melatonin precursor), melatonin synthesis enzyme activity, and the inflammatory cytokine reduction that improves sleep architecture. For comprehensive sleep strategies: Home Remedies for Better Sleep
⚗️ VDRs in SCN (master clock) + pineal gland | CLOCK + BMAL1 circadian gene regulation | 2017 RCT: correcting deficiency significantly improved sleep quality and duration
Pancreatic beta cells — the insulin-producing cells — express VDRs. Vitamin D directly stimulates insulin secretion and improves the sensitivity of insulin receptors in peripheral tissue. Multiple large studies consistently show that lower Vitamin D levels are associated with higher HbA1c, greater insulin resistance, and increased type 2 diabetes risk. A 2019 meta-analysis confirmed Vitamin D supplementation significantly improved insulin sensitivity and reduced HbA1c in Vitamin D-deficient individuals. Given that India has the world’s second-largest diabetic population — and that Vitamin D deficiency simultaneously reduces insulin secretion and impairs insulin sensitivity — correcting Vitamin D deficiency is a genuinely meaningful diabetes prevention and management strategy. The combination of VDR in beta cells + VDR in insulin receptor pathway + VDR in immune cells (reducing the autoimmune beta cell destruction in Type 1 diabetes) makes Vitamin D uniquely relevant to glycaemic health.
⚗️ VDRs in pancreatic beta cells → insulin secretion regulation | 2019 meta-analysis: supplementation improved insulin sensitivity + reduced HbA1c in deficient individuals | India: 2nd largest diabetic population + 70% Vitamin D deficient
Excessive sweating of the head and scalp — particularly at night or in response to mild warmth — is one of the oldest documented and most specific early signs of Vitamin D deficiency, recorded in medical literature for over 100 years as a sign of rickets (the severe deficiency disease) in infants. In adults, it presents as noticeably increased head sweating at rest or during sleep — not the general sweating associated with fever or exertion, but a specific and unexplained scalp and forehead sweating. The mechanism is not fully elucidated but appears to involve Vitamin D’s role in regulating the autonomic nervous system’s sweating response and possibly central thermoregulatory signalling. While less well-studied than the musculoskeletal and immune signs of deficiency, its specificity makes it a useful clinical indicator — particularly when combined with fatigue and bone aching.
⚗️ Documented in rickets literature since early 1900s | Autonomic thermoregulation involvement | Specificity for deficiency — not a general sweating disorder
Skin cells — keratinocytes — express VDRs and can locally synthesise active Vitamin D (1,25-dihydroxyvitamin D) independent of the kidney, using UVB directly for wound healing purposes. Vitamin D regulates keratinocyte proliferation and differentiation (critical for skin barrier repair), the production of antimicrobial peptides at the wound site (defending against infection during the vulnerable healing period), and the transition from inflammatory to proliferative and remodelling phases of wound healing. Deficiency impairs all three stages: barrier repair is slower, infection risk at wound site is higher, and scar remodelling is suboptimal. A 2014 study confirmed significantly lower Vitamin D in patients with chronic wounds that failed to heal normally. People with diabetes — already at high Vitamin D deficiency risk — have doubly impaired wound healing from both the Vitamin D deficiency and the vascular/neuropathic damage of diabetes itself.
⚗️ Keratinocytes express VDRs + locally synthesise active D | Antimicrobial peptide production at wound site | 2014: lower Vitamin D in chronic non-healing wound patients
Vitamin D directly suppresses the expression of renin — the enzyme that initiates the renin-angiotensin-aldosterone system (RAAS), the primary blood pressure-raising hormonal cascade. VDR knockout mice develop hypertension through RAAS overactivation. Multiple human studies confirm inverse associations between Vitamin D levels and blood pressure — lower Vitamin D consistently predicts higher blood pressure. A 2013 meta-analysis found Vitamin D supplementation significantly reduced both systolic and diastolic blood pressure in deficient hypertensive individuals. Given India’s rising hypertension epidemic — affecting approximately 29% of adults — and the 70% Vitamin D deficiency prevalence, the intersection of these two conditions represents a significant and underaddressed treatment opportunity. Correcting Vitamin D deficiency as part of hypertension management has the potential to reduce medication requirements in Vitamin D-deficient hypertensive patients.
⚗️ VDR → renin gene suppression | VDR knockout: hypertension via RAAS | 2013 meta-analysis: D supplementation reduced SBP + DBP in deficient hypertensives
The brain is a major target organ for Vitamin D — VDRs are expressed throughout the brain in neurons, microglia, and astrocytes. Vitamin D regulates the production of nerve growth factor (NGF) and GDNF (glial cell-derived neurotrophic factor) — proteins essential for neuronal survival and synaptic plasticity (the molecular basis of learning and memory). It also provides neuroprotection by reducing oxidative stress and neuroinflammation in brain tissue. Multiple studies associate low Vitamin D with cognitive decline, poor working memory, and increased dementia risk. A 2014 study (Neurology) found that severely Vitamin D deficient individuals were 2.25 times more likely to develop dementia and 2.22 times more likely to develop Alzheimer’s disease over 6 years. The brain fog — difficulty concentrating, word-finding problems, mental sluggishness — that many Vitamin D-deficient Indians experience is the subtle early expression of this neurological impact.
⚗️ VDRs in neurons, microglia, astrocytes | NGF + GDNF regulation → synaptic plasticity | 2014 Neurology: severe deficiency = 2.25x dementia risk + 2.22x Alzheimer’s risk over 6 years
Vitamin D receptors are expressed in ovarian tissue, the uterus, and the pituitary gland — Vitamin D directly influences reproductive hormone production and signalling. In PCOS specifically: Vitamin D deficiency worsens insulin resistance (increasing androgen production through hyperinsulinaemia), reduces AMH (anti-Müllerian hormone) regulation, and impairs follicular development. Multiple studies confirm significantly lower Vitamin D in women with PCOS compared to controls, and supplementation studies show that correcting deficiency improves menstrual regularity, reduces testosterone, and improves insulin resistance in PCOS. Given PCOS affects 22.5% of Indian women — and the high prevalence of Vitamin D deficiency in this same population — Vitamin D testing and correction is an essential part of PCOS management. For the complete PCOS guide: PCOD Problem in Women
⚗️ VDRs in ovarian tissue + pituitary | Insulin resistance worsening → androgen excess | PCOS studies: significantly lower Vitamin D | Supplementation: improved menstrual regularity + reduced testosterone
How to Fix Vitamin D Deficiency Naturally — The Three-Part Protocol
Part A — Sunlight: The Original Source
| Factor | What You Need to Know | India-Specific Guidance |
|---|---|---|
| Time of day | UVB available only when sun is above 45° from horizon — approximately 10am–2pm in India | Morning walks before 10am produce minimal Vitamin D despite being “sunny” — the UVB angle is insufficient |
| Duration | Fair skin: 10–15 min. Medium brown skin: 20–30 min. Dark brown skin: 30–60 min. | Most urban Indians need 30–45 min of peak-hour direct sun for adequate synthesis — practically impossible for office workers |
| Skin exposure | Arms, legs, and back exposed (not just face and hands). Clothing, glass, and sunscreen SPF 30+ block UVB. | Traditional Indian clothing covering most of the body means even outdoor workers may not expose sufficient skin area |
| Frequency | Daily or near-daily — Vitamin D produced is stored but depletes within 2–3 weeks without replenishment | Monsoon months (June–September): sun exposure inadequate even when attempted — supplementation is essential during this period |
| Air pollution caveat | Particulate pollution absorbs and scatters UVB — significantly reducing effectiveness in urban areas | In Delhi, Mumbai, and Kolkata: outdoor sun in heavily polluted conditions produces less Vitamin D than equivalent time in rural areas |
| Do NOT burn | Sunburn produces acute DNA damage and increases skin cancer risk. Vitamin D synthesis plateaus — burning adds no more D but adds cancer risk | Short regular sun exposure without burning is optimal. Gradual tan is protective — it is the burn that damages |
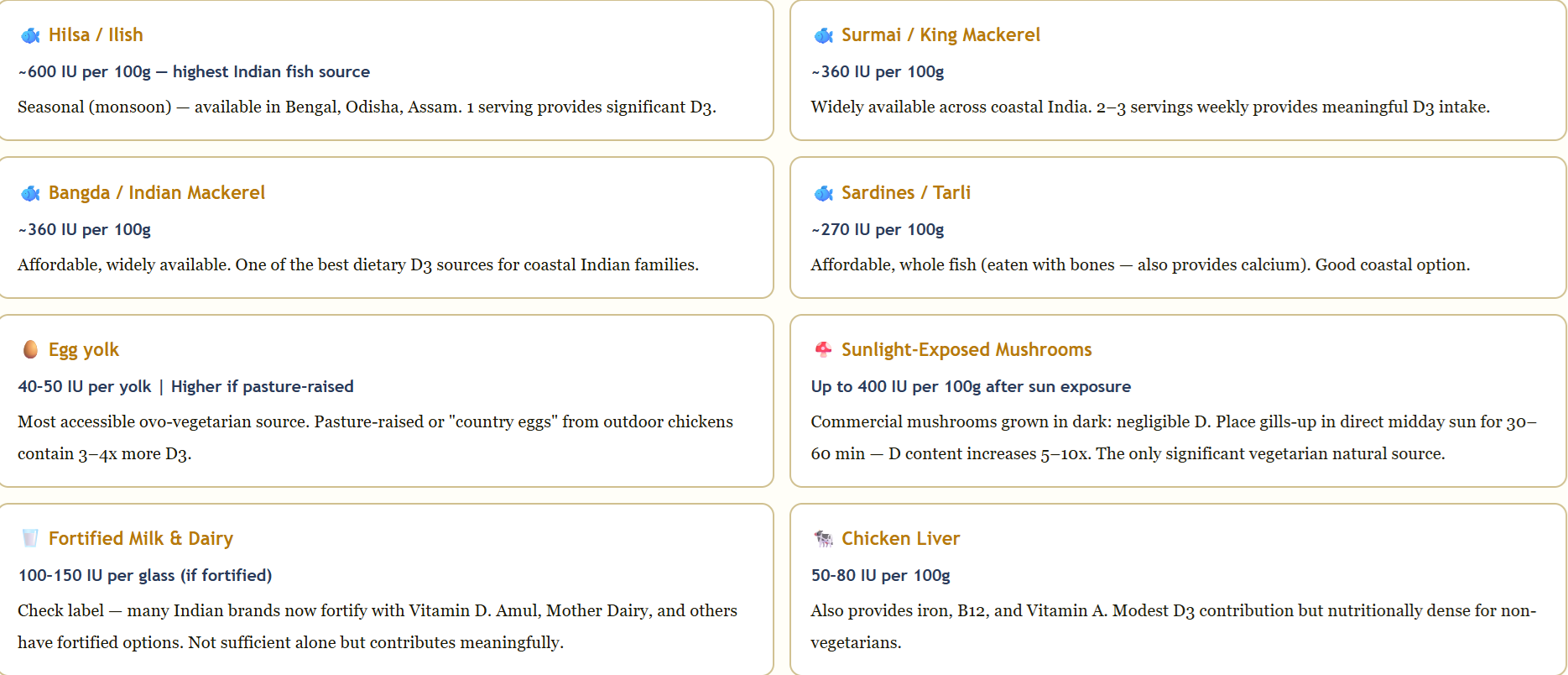
Part B — Food Sources: Limited But Meaningful
Part C — Supplementation: The Most Reliable Correction Tool
Step 1 — Test first: Request 25-OH Vitamin D blood test. Note your exact level.
Step 2 — Correction phase: If below 20 ng/mL: 4,000 IU D3 daily (or 60,000 IU weekly sachet under doctor supervision) for 8–12 weeks. If 20–30 ng/mL: 2,000–3,000 IU D3 daily for 8 weeks.
Step 3 — Essential companions: Vitamin K2 (MK-7) 100–200mcg daily + Magnesium glycinate 300–400mg daily. These are non-optional — D3 without K2 sends calcium to arteries; D3 without magnesium cannot be activated.
Step 4 — Retest at 3 months: Confirm level has reached 40–60 ng/mL. Adjust dose if needed.
Step 5 — Maintenance forever: 1,000–2,000 IU D3 daily indefinitely for most urban Indians, given the structural reasons (indoor lifestyle, covered clothing) that deficiency recurs without ongoing supplementation.
Vitamin D Myths vs. Facts
“If I live in a sunny country, I cannot be Vitamin D deficient.”
Vitamin D requires direct skin exposure to UVB radiation — not ambient warmth or light. 70% of urban Indians are deficient despite living in a tropical country, because indoor lifestyles, covered clothing, high melanin, glass windows, and air pollution prevent adequate UVB reaching the skin. Sunshine is available; the conditions for Vitamin D synthesis from that sunshine are not.
“My blood test said my Vitamin D is normal — I must be fine.”
Lab “normal” for 25-OH Vitamin D (typically above 20 ng/mL) reflects the minimum to prevent rickets — not the optimal range for immune function, mood, muscle strength, and cardiovascular health (40–60 ng/mL). A level of 22 ng/mL is lab “normal” but physiologically insufficient. Always look at your actual number. Also check which Vitamin D was tested — only 25-OH Vitamin D is the correct test.
“I take Vitamin D supplements so my Vitamin D must be fine.”
Vitamin D3 from supplements cannot be activated without magnesium (required for both liver and kidney hydroxylation steps). If you are taking D3 but feeling no improvement and testing shows levels not rising — magnesium deficiency is the most likely explanation. Always combine D3 with magnesium and K2. Test 3 months after starting supplementation to confirm your level has actually risen.
“More is always better — I’ll take 10,000 IU daily.”
Vitamin D toxicity (hypervitaminosis D) is real — it occurs when serum 25-OH Vitamin D exceeds approximately 150 ng/mL from sustained over-supplementation. Symptoms: nausea, weakness, increased urination, kidney stones, calcium deposits in soft tissues. Test before supplementing. The therapeutic range for correction is 2,000–4,000 IU daily — not 10,000 IU for months without testing. Test at 3 months to confirm you are in the optimal range.
Frequently Asked Questions
The 12 signs: deep bone and muscle aching (worse in morning, particularly shins/back/ribs), persistent fatigue not resolved by sleep, frequent illness and slow recovery, low mood and depression, hair loss and thinning, poor sleep quality, worsening blood sugar and insulin resistance, excessive head sweating, slow wound healing, high blood pressure, brain fog and cognitive difficulties, and worsening PCOS or menstrual irregularity. These span multiple body systems because VDRs are expressed in virtually every tissue. If you check 5 or more — test your 25-OH Vitamin D level.
The India paradox explained: indoor office lifestyles (no direct UVB exposure), glass windows block UVB completely, high melanin requires 3–6x longer sun exposure than fair skin, traditional clothing covers most skin, heavy urban air pollution blocks UVB further, predominantly vegetarian diet has no dietary D3 source, and magnesium deficiency (simultaneously prevalent) blocks D3 activation. The result: sunlight is available but the conditions for Vitamin D synthesis are absent for most urban Indians. Supplementation is necessary, not optional.
For correction of deficiency (below 20 ng/mL): 4,000 IU D3 daily for 8–12 weeks (or 60,000 IU weekly sachet under medical supervision). For insufficiency (20–30 ng/mL): 2,000–3,000 IU daily for 8 weeks. For maintenance (above 30 ng/mL): 1,000–2,000 IU daily. Always with Vitamin K2 (100–200mcg MK-7) and Magnesium glycinate (300–400mg). Test at 3 months. Target: 40–60 ng/mL for optimal health outcomes.
Vitamin D3 (from sun or supplement) cannot be activated without magnesium. Two hydroxylation steps — liver (25-hydroxylation) and kidney (1-hydroxylation) — both require magnesium-dependent cytochrome P450 enzymes. If magnesium is deficient (which it is in most Indians), D3 accumulates in its inactive form and produces no physiological benefit. This is why millions of Indians taking D3 supplements feel no improvement. The fix: always combine D3 with magnesium glycinate or citrate 300–400mg daily. For full magnesium guide: What Magnesium Deficiency Does to Your Body
For most urban Indians: practically no. The conditions required (direct skin exposure of arms and legs, 10am–2pm, 30–45 minutes for darker skin tones, daily) are unachievable for most office workers, and urban air pollution further reduces UVB effectiveness. Exceptions: outdoor workers with large skin exposure in rural areas with clear skies. Even for them: testing is advisable, because combined with the vegetarian diet’s lack of D3, their levels may still be suboptimal. For urban Indians: supplementation is necessary, not optional, particularly through the monsoon months when sun exposure drops further.
Related Articles You’ll Love
Vitamin D is not a vitamin you find in food. It is a hormone your skin makes from sunlight — a hormone that your body expects because for 99.9% of human evolutionary history, people spent their days outdoors. The urban Indian office worker spending 10 hours indoors, under glass, in covered clothing, in an air-conditioned building in a polluted city has removed every component of that evolutionary expectation. The body did not adapt to this in 50 years. The symptoms — aching bones, tired muscles, frequent illness, low mood, hair loss — are the body signalling the absence of something it requires.
The fix is simple: test, supplement D3 with K2 and magnesium, get outside during peak UVB hours when possible, eat fatty fish or sun-exposed mushrooms. Give it 12 weeks. Retest. The transformation in how you feel — particularly if your level was severely low — is often described by patients as one of the most significant health improvements they have experienced.
Test first. Fix what you find. Then go stand in the sun between 10am and 2pm — even for 15 minutes. Your cells are waiting. ☀️Which sign resonated most — the bone aching you assumed was arthritis, the fatigue that sleep never fixes, or the fact that your Vitamin D supplements haven’t worked because you were taking them without magnesium? Share this with every Indian who’s been told their tests are “normal” but they still feel unwell. 👇
Sources & Further Reading
- BMJ (2017) — Vitamin D Supplementation Meta-analysis (25 RCTs, 11,321 participants): 12% Reduction in Respiratory Infection Risk; 50% in Severely Deficient Individuals
- Neurology (2014) — Vitamin D Deficiency and Dementia: 2.25x Higher Risk of Dementia; 2.22x Higher Alzheimer’s Risk Over 6 Years
- Nutrients (2018) — Magnesium and Vitamin D: Both D3 Hydroxylation Steps Require Magnesium-Dependent Enzymes — Deficiency Renders Supplementation Ineffective
- Sleep Medicine Reviews (2018) — Vitamin D and Sleep: Deficiency Significantly Associated with Poor Sleep Quality, Short Duration, and Impaired Efficiency
- Dermatology Research and Practice (2013) — Vitamin D and Hair Loss: Significantly Lower Levels in Women with Telogen Effluvium and Female Pattern Hair Loss
- Molecular and Cellular Endocrinology (2014) — Vitamin D and PCOS: Supplementation Improved Menstrual Regularity and Insulin Resistance
- Journal of Human Hypertension (2013) — Vitamin D and Blood Pressure: Supplementation Significantly Reduced SBP and DBP in Deficient Hypertensive Individuals
- HerbeeLife — Why Your Body Aches All the Time: Vitamin D and Pain Science
- HerbeeLife — Natural Health & Ayurvedic Wellness
Disclaimer: This content is for informational and educational purposes only. Vitamin D supplementation, particularly at high doses, should be undertaken with appropriate blood testing and ideally under medical supervision. Never self-prescribe high-dose Vitamin D without knowing your baseline level. Read full disclaimer →

