Dengue can be fatal. This article covers supportive home care for mild dengue cases under medical supervision. It is not a substitute for medical diagnosis and treatment.
See a doctor immediately if you have high fever with severe joint/muscle pain, pain behind the eyes, or rash — dengue testing and monitoring are essential.
Go to hospital immediately if you develop: severe abdominal pain, persistent vomiting, any bleeding, extreme fatigue, cold/clammy skin, or if your platelet count is falling rapidly. See the full warning signs section below.
Never take ibuprofen, aspirin, or naproxen for dengue fever — these NSAIDs inhibit platelet function and increase bleeding risk, which can be life-threatening in dengue. Use only paracetamol (acetaminophen) for fever control, under medical guidance.
The key word throughout this guide is supportive. There is no home cure for dengue. There is no herb that stops the viral replication or replaces IV fluid management for severe cases. But there is meaningful evidence-backed supportive care that helps the body manage dengue safely — and critically, there is the knowledge of when supportive care is no longer sufficient and hospital admission is urgent. This guide gives you both.
What Dengue Actually Is — The Biology You Need to Understand
Dengue fever is caused by the dengue virus (DENV) — a single-stranded RNA flavivirus with four distinct serotypes: DENV-1, DENV-2, DENV-3, and DENV-4. All four circulate in India. Infection with one serotype confers lifelong immunity to that serotype — but not to the others. A second infection with a different serotype is typically more severe due to a phenomenon called antibody-dependent enhancement (ADE): antibodies from the first infection bind to the new virus but cannot neutralise it, instead facilitating its entry into immune cells and amplifying viral replication. This is why second dengue infections carry significantly higher risk of severe disease than first infections.
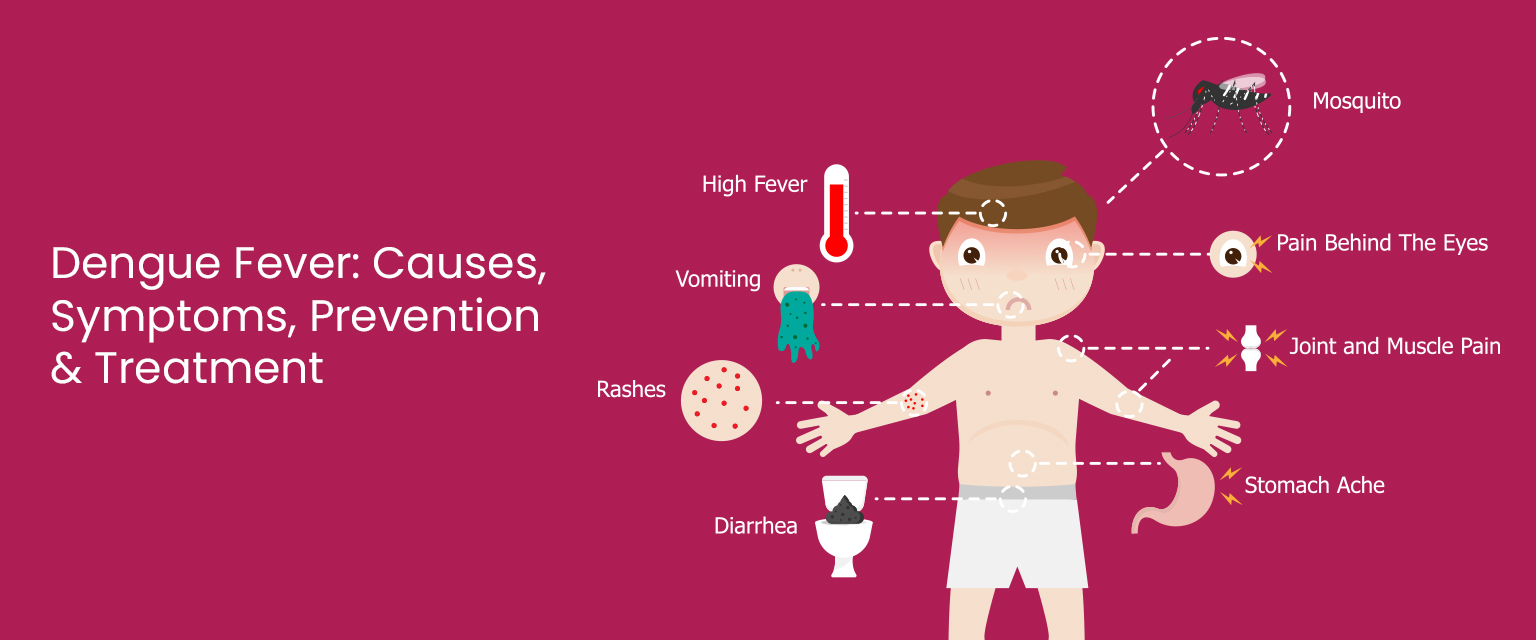
The primary vector is Aedes aegypti — a small, dark mosquito with distinctive white banding on its legs. Unlike the malaria mosquito (Anopheles), Aedes bites primarily during the day — especially in the two hours after sunrise and the two hours before sunset. It breeds in small collections of clean, stagnant water: flower pots, water tanks, tyres, cooler trays, overhead tanks, and even bottle caps — making it uniquely well-adapted to urban Indian environments.
Fever: The dengue virus replicates in monocytes, macrophages, and dendritic cells, triggering a massive cytokine release (interferon-α, TNF, IL-6, IL-10) — the systemic inflammatory response that produces the characteristically high, sudden fever.
Severe joint and muscle pain (“breakbone fever”): Viral replication in muscle tissue combined with prostaglandin-driven inflammation from the cytokine storm produces the most intense myalgia and arthralgia of any common viral illness — the extreme pain that gives dengue its descriptive name.
Thrombocytopaenia (falling platelet count): The dengue virus infects megakaryocytes (platelet-producing bone marrow cells), directly reducing platelet production. Simultaneously, platelet-antibody complexes form, and cross-reactive antibodies attack platelets. The endothelial damage from the viral infection also causes platelet consumption at damaged vessel walls. The combined effect: platelet counts can fall from a normal 1.5–4 lakh/mm³ to critically low levels (<20,000/mm³) within days.
Plasma leakage (the defining feature of severe dengue): In severe dengue, the cytokine storm increases vascular permeability — fluid leaks from blood vessels into surrounding tissue. This produces haemoconcentration in the blood, plasma accumulation in the chest and abdomen (pleural effusion, ascites), and circulatory collapse (dengue shock syndrome) if uncorrected. This is the mechanism behind the life-threatening phase — and why IV fluid management in hospital is the cornerstone of severe dengue treatment.
The Three Phases of Dengue — Why Phase 2 Is the Danger Window
Understanding dengue’s three clinical phases is the most important knowledge in this guide. Most dengue deaths and serious complications occur because families don’t know that the period when fever drops is the most dangerous — not the safest.
What happens: Sudden high fever 39–40°C, severe headache, retro-orbital pain, intense joint/muscle pain, nausea, vomiting, and flushing. Rash may begin to appear. Platelet count begins falling.
Management: Medical evaluation + dengue test. Paracetamol for fever. Aggressive oral hydration. Rest. Mosquito protection (to prevent spreading to other mosquitoes). Monitor daily platelet count from day 2.
What happens: Fever drops or disappears — creating the false impression of recovery. This is when plasma leakage peaks. Platelet count reaches its lowest. Severe dengue complications (haemorrhage, shock) develop in this phase — precisely when families often relax and stop monitoring.
Management: Close clinical monitoring even though fever has gone. Watch for warning signs (see below). Most hospitalisations occur in this phase. If warning signs appear — hospital immediately. Do NOT assume recovery because fever dropped.
What happens: Plasma reabsorption, platelet count recovery (can overshoot normal briefly). Appetite returns. Rash may resolve. Significant fatigue may persist for 2–4 weeks even after acute illness resolves.
Management: Continue hydration and nutrition support. Nutritious easily digestible foods. Gradual return to activity. Monitor for bradycardia (slow heart rate) which can occur during recovery. Platelet transfusion virtually never needed in recovery phase — platelet count recovers naturally.
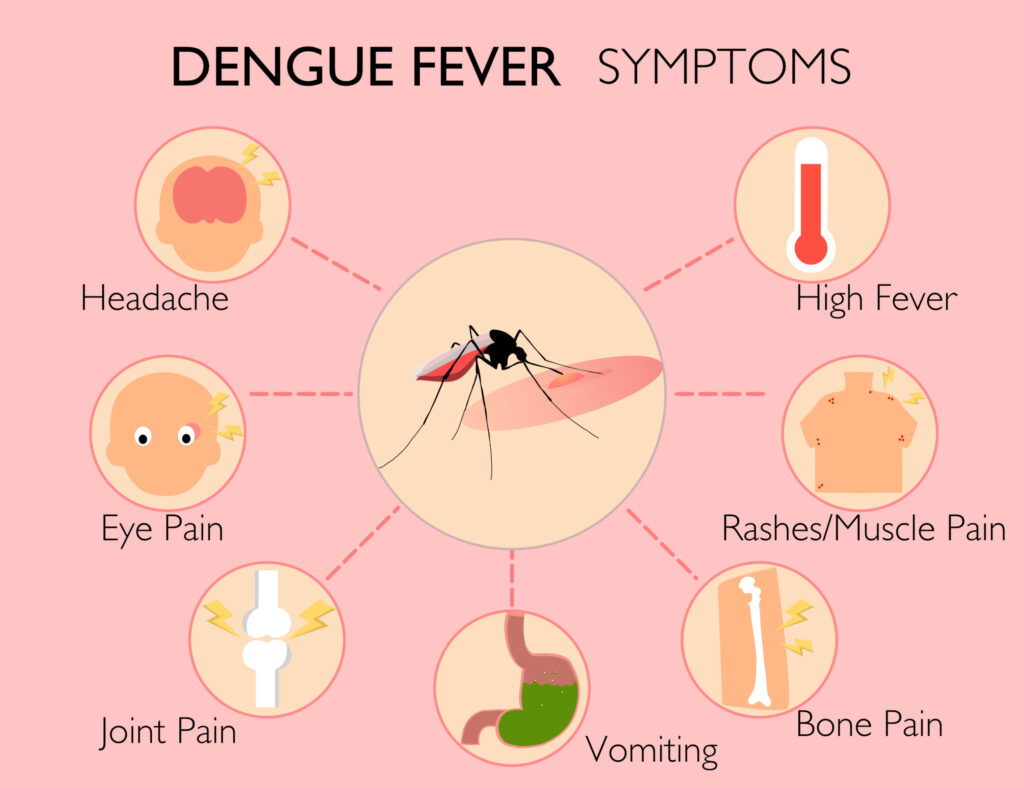
Dengue Fever Symptoms — Complete Guide to Recognising and Monitoring
Dengue fever is characteristically sudden in onset — going from feeling well to 39–40°C (102–104°F) within hours. The dengue fever pattern is sometimes described as “saddle-back” — an initial fever that may briefly drop and then return — though this pattern is not universal. The fever typically lasts 2–7 days. The sudden, high-grade onset following a mosquito-dense environment or travel during dengue season should immediately prompt dengue testing (NS1 antigen test positive in days 1–5; IgM antibody test positive from day 5 onward).
What NOT to take: Aspirin, ibuprofen, and naproxen are absolutely contraindicated in dengue — they impair platelet function (through COX-1 inhibition) and can cause life-threatening bleeding in the context of dengue thrombocytopaenia. Use only paracetamol (500mg–1g four-hourly, maximum 4g/day in adults) under medical guidance.
⚗️ NS1 antigen: days 1–5 | IgM: from day 5 | Paracetamol only — NEVER NSAIDsPain behind the eyes — classically worsened by eye movement — is one of the most characteristic symptoms of dengue fever, and helps distinguish it from other viral fevers. The mechanism involves the periorbital tissues’ rich blood supply responding to the inflammatory cytokine cascade of dengue. This symptom, combined with severe headache, fever, and myalgia, is highly suggestive of dengue and should prompt testing immediately.
⚗️ Retro-orbital pain: distinguishing dengue feature from other viral feversThe severe musculoskeletal pain of dengue — giving it the historical name “breakbone fever” — is caused by viral replication in muscle and connective tissue cells combined with the prostaglandin and cytokine-driven systemic inflammation of the dengue immune response. The pain affects muscles, joints, and bones simultaneously and is typically rated by patients as among the most severe pain they have experienced. It is disproportionately severe compared to a regular viral fever and may be the first indicator that the illness is not a simple flu.
⚗️ Viral myositis + cytokine-driven inflammation | Most severe myalgia of common viral illnessesThe dengue rash typically appears on days 3–5 of illness — after fever onset. It is a maculopapular rash — flat red areas with raised bumps — that may appear over most of the body (trunk, extremities, face) and is often described as “islands of white in a sea of red.” It may be itchy. A second rash can appear in the recovery phase (days 7–8) as platelet recovery begins — characterised by petechiae (tiny red dots from small bleeds) on the feet and lower legs.
The rash is a useful clinical marker but should not be waited for before seeking evaluation — dengue testing should be done with any combination of high fever + severe headache + joint/muscle pain + retro-orbital pain, regardless of whether rash has appeared.
⚗️ Maculopapular rash days 3–5 | “Islands of white in sea of red” | Recovery petechiae on lower limbsThe dengue platelet count fall is among the most medically significant and practically important aspects of dengue management for families. Normal platelet count: 1.5–4.5 lakh (150,000–450,000) per mm³. In dengue, counts typically start falling around day 3–4 and reach their nadir (lowest point) around day 6–7, then recover from day 8 onward.
| Platelet Count | Clinical Status | Action Required |
|---|---|---|
| >1 lakh (100,000) | Monitoring phase | Oral hydration, rest, daily monitoring, outpatient management usually appropriate |
| 50,000–1 lakh | Watch closely | Medical review essential, close monitoring, consider hospitalisation especially if falling rapidly |
| 20,000–50,000 | High risk | Hospitalisation strongly indicated, strict rest, avoid any injury risk |
| <20,000 | Critical | Hospital admission mandatory, platelet transfusion may be considered (only if active bleeding or critical procedure needed) |
Critical misconception: Platelet transfusion is NOT the routine treatment for low platelet count in dengue — it is only indicated for active significant bleeding or when a surgical procedure is urgently needed. Most platelet counts recover spontaneously. Premature or unnecessary platelet transfusion carries its own risks (transfusion reactions, volume overload) and is widely overused in Indian dengue management. Follow your treating doctor’s guidance specifically.
⚗️ Nadir day 6–7 | Platelet transfusion NOT routine — only for active bleeding | Spontaneous recovery from day 8⚠️ Warning Signs of Severe Dengue — Go to Hospital Immediately
Severe abdominal pain or tenderness: Indicates plasma leakage around the liver or internal haemorrhage. Severe abdominal pain in dengue is a medical emergency — do not wait and monitor at home.
Persistent vomiting (3+ episodes in 24 hours or inability to keep any fluids down): Causes dangerous dehydration and prevents essential oral hydration. Requires IV fluid administration at hospital.
Any bleeding: Blood in vomit (haematemesis), black tarry stool (melaena), blood in urine (haematuria), significant nosebleed, bleeding gums, or petechial haemorrhage spreading rapidly.
Rapid breathing or difficulty breathing: May indicate pleural effusion (fluid around the lungs from plasma leakage). Requires urgent assessment.
Extreme fatigue AND restlessness together: The combination of extreme tiredness with agitation or restlessness is a clinical sign of poor tissue perfusion — early shock. Seek emergency care immediately.
Cold or clammy skin, pale appearance: Signs of circulatory compromise — blood is being redirected to vital organs. This is early dengue shock syndrome. Emergency.
Confusion or altered consciousness: Brain is not being adequately perfused. Medical emergency.
Sudden improvement in the first week followed by feeling very unwell again: The “double sickening” of dengue — fever drops (looks like recovery) then severe complications develop in the critical phase. This is the most dangerous time.
Dengue in vulnerable groups — lower threshold for hospitalisation: Infants and young children (under 5), elderly (over 65), pregnant women (dengue can cause foetal complications), and those with diabetes, heart disease, kidney disease, or on blood thinners should have a much lower threshold for hospital admission — consult your doctor at first dengue diagnosis, not when warning signs appear.
Supportive Home Care for Mild Dengue — Evidence-Backed, Medically Appropriate
Important framing: The following supportive measures are appropriate for mild dengue — patients with confirmed or suspected dengue who have been evaluated by a doctor, have platelets above 1 lakh, no warning signs, and are able to take adequate oral fluids. They are not appropriate as sole management for moderate or severe dengue. Daily monitoring and medical follow-up remain essential throughout.
Adequate fluid intake is the cornerstone of dengue supportive care — and the most important measure a family can implement at home. Dengue causes fluid loss through high fever, sweating, vomiting, and reduced intake. In the critical phase, plasma leakage reduces intravascular volume. Adequate hydration maintains circulating volume, supports kidney function for viral clearance, and prevents the dehydration that can accelerate progression to shock.
The WHO dengue guidelines recommend oral rehydration at 2–3 litres daily for adults with mild dengue — more if fever is high or vomiting is occurring. Coconut water (nariyal paani) is specifically valuable: it provides electrolytes (potassium, sodium, magnesium) in proportions close to oral rehydration salts, and its isotonicity makes it one of the most effective natural hydration vehicles available. A 2009 study confirmed coconut water’s hydration efficacy comparable to commercial electrolyte beverages in rehydration scenarios.
Of all the traditional Indian remedies for dengue, papaya (Carica papaya) leaf juice has the strongest clinical evidence. A 2013 randomised controlled trial published in Evidence-Based Complementary and Alternative Medicine found that papaya leaf extract significantly increased platelet counts and white blood cell counts in confirmed dengue patients compared to control, with the platelet benefit becoming statistically significant by day 5 of treatment. A 2014 prospective study at a Malaysian hospital found similar results.
The proposed mechanisms are multiple: papaya leaves contain flavonoids (quercetin, kaempferol) that may stimulate megakaryocyte activity (platelet production), acetogenin compounds (particularly carpaine) that have demonstrated antiviral activity against dengue virus in vitro, and Vitamin C that supports immune function and capillary integrity. The enzyme papain has anti-inflammatory properties relevant to dengue’s cytokine-driven inflammation. Importantly, no significant adverse effects were reported in these trials at standard doses.
Critical context: Papaya leaf juice is supportive adjunct therapy — it does NOT replace medical monitoring, hospitalization when indicated, or IV fluids. Use it alongside — never instead of — medical care. Several small RCTs showing benefit do not mean dengue can be managed at home with papaya leaf alone.
Giloy (Tinospora cordifolia, also called guduchi or amrita) is among the most revered herbs in Ayurveda for immune support — and has specific dengue-relevant clinical research. A 2014 randomised trial published in the Journal of Vector Borne Diseases found that giloy stem extract significantly improved platelet count recovery and reduced fever duration in dengue patients compared to standard treatment alone. The active compounds — tinosporine, berberine, and various alkaloids — have immunomodulatory, anti-inflammatory, and platelet-stimulating properties documented in pharmacological research.
Giloy works through multiple mechanisms relevant to dengue: stimulating macrophage activity (improving dengue viral clearance), reducing pro-inflammatory cytokine production (addressing the cytokine storm driving dengue pathology), and potentially supporting megakaryocyte activity (platelet production). It is considered one of the safest Ayurvedic herbs for sustained use.
Tulsi (Ocimum sanctum) has documented antiviral, immunomodulatory, and anti-inflammatory properties directly relevant to dengue management. Ursolic acid and oleanolic acid in tulsi inhibit dengue viral protease — a key enzyme required for dengue replication — in laboratory studies. Eugenol, the primary volatile compound, reduces pro-inflammatory cytokine production relevant to the dengue cytokine storm. Multiple animal model studies confirm tulsi’s anti-dengue viral activity, and its immunomodulatory effects are well-established in human clinical research.
A 2017 study in the Journal of Ethnopharmacology confirmed tulsi’s antiviral activity against flaviviruses (the family dengue belongs to), with eugenol specifically showing inhibitory activity. In Ayurvedic tradition, tulsi-ginger-black pepper decoction (kadha) has been the standard Indian home intervention for febrile viral illness for millennia — and the pharmacological basis for its dengue relevance is now being understood.
Nutritional support during dengue serves two goals: providing energy for immune function and recovery without stressing a digestive system weakened by viral illness, and specifically supporting platelet recovery and vascular integrity. During the febrile phase, appetite is typically absent — small, frequent, easily digestible foods are most appropriate. As fever reduces, gradually increasing nutritional density supports recovery.
Phase 1 (febrile phase) — easiest to digest: Dal khichdi (moong dal and rice — easy to digest, protein + carbohydrate + hydration), rice kanji/congee (warm rice water — extremely gentle on the stomach), fresh coconut water (hydration + electrolytes), warm dal soup (protein + hydration), fresh pomegranate juice (polyphenols + iron for blood cell recovery — particularly relevant for haemorrhagic dengue), and guava (high Vitamin C for immune function).
Phase 3 (recovery) — building back: Increase to normal sattvic whole foods. Amla (highest Vitamin C for immune restoration), drumstick/moringa (iron + vitamins for post-dengue anaemia recovery), methi and palak (iron-rich), protein-rich dal and legumes (muscle recovery from severe myalgia), and fresh seasonal fruits. Continue avoiding alcohol for at least 2 weeks post-recovery — liver enzyme elevation from dengue takes time to normalise.
⚗️ Pomegranate polyphenols: antioxidant + haematopoietic support | Guava Vitamin C: immune function | Gradual nutritional progressionNeem (Azadirachta indica) has well-documented antiviral properties — nimbin, nimbidin, and gedunin demonstrate inhibitory activity against several viral pathogens in laboratory research. A 2012 study found neem leaf extracts inhibited dengue virus replication in cell culture through multiple mechanisms including inhibition of viral entry and replication. In Ayurveda, neem is classified as a tikta (bitter) herb with anti-inflammatory, antipyretic, and immune-enhancing properties.
Traditional preparation: boil 10–12 fresh neem leaves in water, strain, and drink the decoction (1 cup once daily). The bitterness can be moderated with a small amount of honey. Alternatively, neem churna (powder) ½ tsp in warm water. Neem should be used in moderate, time-limited amounts during dengue illness — long-term high-dose neem has hepatotoxic potential in some individuals, though short-term therapeutic use is considered safe in Ayurvedic tradition.
⚗️ Nimbin + gedunin: dengue viral replication inhibition (in vitro 2012) | Antipyretic in Ayurvedic traditionComplete bed rest during the febrile and critical phases of dengue is essential — not optional. The severe myalgia of dengue makes movement painful, but the physiological rationale goes beyond comfort. Physical activity during dengue increases metabolic demand at precisely the moment the body’s circulatory capacity is most compromised; it can elevate heart rate in a compromised cardiovascular system; and in the context of thrombocytopaenia, any fall or physical injury carries bleeding risk that would be manageable with normal platelet counts but potentially life-threatening with counts below 50,000.
Mosquito net during illness: This is a critical public health measure that is frequently overlooked — a person with dengue fever is viraemic (has dengue virus circulating in their blood). If an Aedes mosquito bites a dengue patient and then bites another person, it transmits dengue. Using a mosquito net or insect repellent during illness prevents the dengue patient from becoming a source of infection for household members and neighbours. Dengue mosquitoes bite during the day — protection is needed throughout the day, not just at night.
⚗️ Viraemia → mosquito transmission prevention during illness | Bleeding risk with thrombocytopaenia + physical injuryDengue Prevention — Eliminating Breeding Sites is the Only Sustainable Solution
1. Eliminate breeding sites weekly: Empty and scrub all water containers weekly — flower pots (the saucer under the pot), cooler trays, overhead tank lids, buckets, tyres, and any container that holds water. Aedes larvae develop from egg to adult mosquito in 7–10 days — weekly emptying breaks the breeding cycle. Scrubbing removes eggs (which stick to container walls and survive drying). This single measure, done consistently by entire neighbourhoods, is more effective than any fumigation or fogging campaign.
2. Covered water storage: All water storage containers must be tightly covered. A mesh cover allows water access while preventing mosquito egg-laying. Overhead tanks — the most overlooked breeding site in urban India — must be completely sealed with properly fitted lids with no gaps.
3. Personal protection during peak mosquito hours: Aedes mosquitoes bite primarily 2 hours after sunrise and 2 hours before sunset — not primarily at night. Apply repellent during these daytime windows. Long sleeves and covered legs are effective during these peak periods. DEET-based repellents are the most effective; picaridin and IR3535 are safer alternatives particularly for children and pregnant women.
4. Larval control in unmovable water bodies: For water bodies that cannot be emptied (roof drains, decorative ponds, tree holes): Bacillus thuringiensis israelensis (BTi) — a biological larvicide available in India — is safe, effective, and environmentally friendly. Temephos (abate) larvicide tablets are another option for large tanks.
5. Community action: Dengue prevention is inherently collective — a single breeding site can produce hundreds of mosquitoes that spread across a neighbourhood. Coordinate with housing societies, RWAs, and local municipal bodies for area-wide elimination campaigns during pre-monsoon and monsoon months.
Dengue Myths vs. Facts — The Ones That Cost Lives in India
“When the fever breaks in dengue, the danger is over.”
When the fever drops (days 3–7), the critical phase BEGINS. Plasma leakage peaks. Platelet count reaches its nadir. Most severe dengue complications and deaths occur in the 24–48 hours after fever drops. Continue vigilant monitoring for warning signs even when — especially when — the fever seems to be improving. This myth kills people every dengue season.
“Take ibuprofen or aspirin to bring down dengue fever fast.”
Ibuprofen, aspirin, and naproxen are absolutely contraindicated in dengue. These NSAIDs inhibit COX-1, impairing platelet function — which, combined with dengue’s own platelet destruction, creates severe bleeding risk. Only paracetamol (acetaminophen) should be used for fever in dengue, under medical guidance. This is one of the most dangerous medical errors made in home dengue management.
“If the platelet count is low, platelet transfusion is urgently needed.”
Platelet transfusion is NOT routinely indicated for low platelet count in dengue — even with counts below 20,000 — unless there is active significant bleeding or an urgent surgical procedure is needed. Platelets recover spontaneously in dengue. Unnecessary transfusions carry their own risks (reactions, volume overload) and are overused in Indian dengue management. Follow your treating physician’s specific guidance on platelet transfusion necessity.
“Second dengue infection is milder than the first because you have antibodies.”
Second dengue infection with a DIFFERENT serotype is typically more severe, not milder, due to antibody-dependent enhancement (ADE). Pre-existing antibodies from the first infection facilitate entry of the new serotype into immune cells, amplifying viral replication. This is why areas with all four serotypes circulating (including most of India) have higher rates of severe dengue than single-serotype endemic regions.
“Dengue testing is unnecessary if symptoms look like dengue.”
Dengue testing is essential for confirmed diagnosis. Malaria, leptospirosis, typhoid, chikungunya, and viral hepatitis can produce similar symptom profiles — and have different management requirements. The NS1 antigen test (positive days 1–5) and IgM antibody test (positive from day 5) are widely available and affordable across India. Testing also enables the platelet monitoring that is essential for safe dengue management.
Frequently Asked Questions About Dengue Fever
Early warning signs of dengue: sudden high fever (39–40°C) appearing 4–10 days after possible mosquito exposure, severe headache particularly behind the eyes (retro-orbital pain), intense joint and muscle pain (‘breakbone fever’), nausea and vomiting, loss of appetite, and rash appearing days 3–5. Get a dengue NS1 antigen test immediately if these symptoms appear during dengue season — do not wait to see if they worsen.
Go to hospital immediately for: severe abdominal pain, persistent vomiting, any bleeding (nose, gums, in vomit or stool, urine), rapid breathing, extreme fatigue combined with restlessness, cold or clammy skin, confusion, and — critically — sudden fever drop during days 3–7 (the critical phase begins when fever breaks). These signs indicate plasma leakage or haemorrhage. Do not wait and monitor at home.
Multiple clinical studies including a 2013 RCT show papaya leaf extract significantly increases platelet and white blood cell counts in dengue patients. The mechanisms include flavonoids (quercetin, kaempferol) stimulating megakaryocyte activity, acetogenin compounds with antiviral activity, and anti-inflammatory effects. It is evidence-backed supportive adjunct therapy — not a replacement for medical monitoring or hospital admission when indicated.
Most important: 2–3 litres of fluid daily — ORS solution, coconut water, rice kanji, dal soup, warm water with lemon and honey. For food during fever phase: easily digestible dal khichdi, rice kanji, fresh coconut water, warm clear soups. In recovery: amla, guava (Vitamin C), pomegranate (antioxidants), moringa/drumstick (iron + vitamins), protein-rich dals. Avoid ibuprofen/aspirin (dangerous in dengue), alcohol (liver stress), and undiluted fruit juices.
Go to hospital immediately for: severe abdominal pain, persistent vomiting, any bleeding, difficulty breathing, extreme fatigue with restlessness, cold/clammy skin, confusion, platelet count below 100,000 and rapidly falling, or any warning signs appearing when the fever drops (days 3–7). Infants, elderly, pregnant women, and those with chronic conditions should consult a doctor at the first sign of possible dengue — not when warning signs appear. Home remedies are for mild dengue under medical supervision only.
Dengue distinguishes itself through: extremely high sudden fever (39–40°C), retro-orbital pain (pain behind the eyes worsened by eye movement), extreme severity of joint and muscle pain beyond typical viral fever, characteristic maculopapular rash appearing days 3–5, and falling platelet count (measured by blood test). A dengue NS1 antigen test (days 1–5) or IgM test (from day 5) confirms the diagnosis. Always test — dengue can look similar to malaria, typhoid, chikungunya, and leptospirosis, each requiring different management.
Related Articles You’ll Love
Dengue is managed at home more often than it should be in India — and hospitalised later than it should be. The two facts every Indian family needs to know: the critical phase starts when the fever breaks, not when it ends; and ibuprofen in dengue is not a pain relief option, it is a bleeding risk. Beyond these two essential truths, the supportive measures — papaya leaf juice, giloy, tulsi kadha, coconut water, rest, and mosquito protection — are backed by a growing body of clinical research.
Your kitchen has real tools. But dengue is a disease that can kill within hours of warning signs appearing. Know the signs. Know the threshold for hospital. Use both.
The most important dengue home remedy is knowing when to stop relying on home remedies. 🌿Share this guide with your family before dengue season — July to November in most of India. The warning signs section alone could save a life. 👇
Sources & Further Reading
- WHO Dengue Guidelines for Diagnosis, Treatment, Prevention and Control (2012)
- Evidence-Based Complementary and Alternative Medicine (2013) — Papaya Leaf Extract RCT: Increased Platelet + WBC Count in Dengue
- Journal of Vector Borne Diseases (2014) — Giloy (Tinospora cordifolia): Improved Platelet Recovery in Dengue Patients RCT
- Journal of Ethnopharmacology (2017) — Tulsi (Ocimum sanctum) Antiviral Activity Against Dengue and Other Flaviviruses
- Virology Journal (2012) — Neem Leaf Extracts: Inhibition of Dengue Virus Replication In Vitro
- Asian Pacific Journal of Tropical Biomedicine (2012) — Dengue Fever: Current Status and Future Perspective in India
- Journal of the International Society of Sports Nutrition (2009) — Coconut Water for Rehydration: Comparable to Commercial Electrolyte Beverages
- HerbeeLife — Health Benefits of Turmeric: Anti-Inflammatory and Antiviral Mechanisms
- HerbeeLife — Natural Health & Ayurvedic Wellness
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Dengue fever is a serious medical condition that requires professional diagnosis and monitoring. If you suspect dengue, see a doctor immediately. If warning signs appear, go to hospital without delay. Never manage dengue solely with home remedies. Read full disclaimer →

