If you have ever experienced the combination of a concrete-filled head, facial pain that worsens every time you bend forward, thick green-yellow mucus, and a headache that no amount of paracetamol fully resolves — you know sinusitis. It is one of the most common reasons for doctor visits globally, one of the most frequent causes of antibiotic prescriptions (most of them unnecessary), and one of the conditions where the gap between what people do (take antibiotics and wait) and what the evidence supports (nasal irrigation, steam, targeted anti-inflammatory remedies) is widest and most consequential.
This comprehensive guide covers everything you need to understand and manage sinusitis effectively — from the anatomy and physiology of why the sinuses become infected, through the four clinical types and their different management implications, to the 12 most evidence-backed home remedies, and the specific Ayurvedic wisdom about Pratishyaya (the Ayurvedic classification of nasal and sinus conditions) that anticipated many of the mechanisms modern ENT medicine now confirms. Most importantly, it covers when natural management is appropriate and when symptoms demand professional medical evaluation.
Understanding Your Sinuses — The Anatomy Behind the Problem
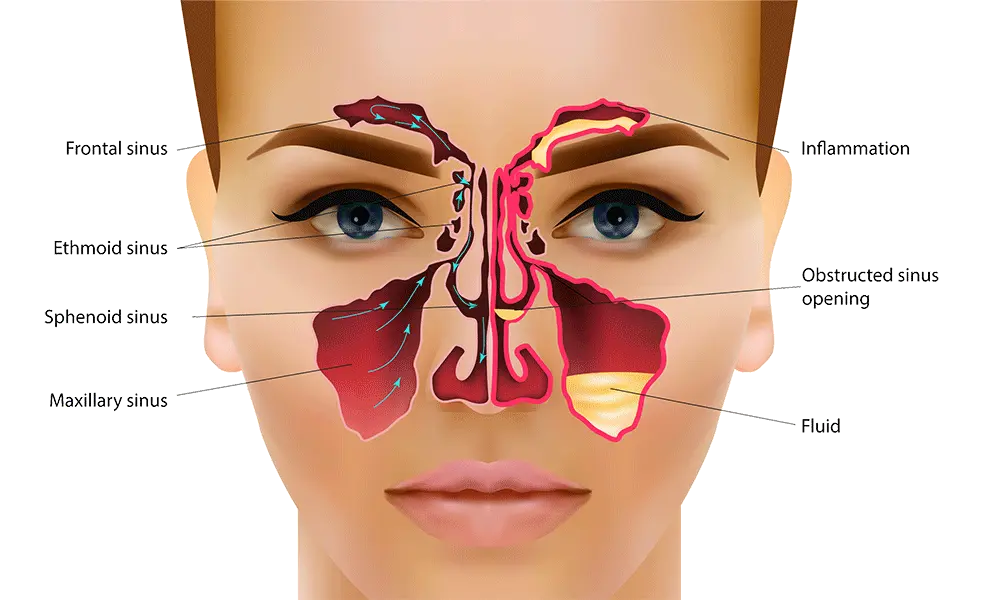
The paranasal sinuses are four paired air-filled cavities within the bones of the skull — the maxillary sinuses (in the cheekbones, the largest pair), frontal sinuses (in the forehead above the eyes), ethmoid sinuses (between the eyes, a complex of small cells), and sphenoid sinuses (deep behind the nose). They are lined with ciliated mucous membrane — the same type of respiratory epithelium that lines the nose, throat, and bronchial airways — and connect to the nasal cavity through small openings called ostia.
The sinuses serve multiple physiological functions: they reduce the weight of the skull, humidify and warm inhaled air, contribute resonance to the voice, and produce mucus that traps inhaled particles and pathogens, which the cilia then sweep toward the ostia for drainage into the nasal cavity and subsequent swallowing or expectoration. This mucociliary clearance system — the continuous movement of the mucous blanket toward the sinus ostia — is the primary defence mechanism of the sinuses against infection.
Sinusitis occurs when this clearance system breaks down. The ostia — remarkably small (1–3mm in diameter) given the volume of mucus they must drain — become obstructed through inflammation and swelling of the surrounding mucosa, typically triggered by a viral upper respiratory tract infection. When drainage is impaired, mucus stagnates in the sinus cavity, oxygen tension falls (creating the anaerobic conditions that favour bacterial overgrowth), and secondary bacterial infection develops in approximately 0.5–2% of viral sinusitis episodes. This pathophysiological sequence is the basis of all effective sinusitis management: anything that reduces mucosal oedema and restores ostial drainage is therapeutic; anything that addresses only symptoms without restoring drainage is temporary at best.
Types of Sinusitis — The Classification That Determines Management
Not all sinusitis is the same — the type determines whether antibiotics are appropriate, whether natural remedies alone are sufficient, and what the likely clinical trajectory will be.
Acute viral rhinosinusitis (AVRS) is the most common form — a self-limiting viral infection of the nasal passages and sinuses, usually lasting 7–10 days and caused by rhinovirus, coronavirus, influenza, parainfluenza, or adenovirus. This is what most people mean when they say they have a “sinus infection.” It does not respond to antibiotics (viruses are not killed by antibiotics), and the evidence-based management is symptomatic: nasal saline irrigation, steam inhalation, adequate hydration, and nasal corticosteroid spray if available. Approximately 98% of acute sinusitis cases are viral and resolve without antibiotics within 10 days.
Acute bacterial rhinosinusitis (ABRS) occurs when bacterial superinfection develops following viral rhinosinusitis — most commonly with Streptococcus pneumoniae, Haemophilus influenzae, or Moraxella catarrhalis. It is suggested by: symptoms that worsen after initial improvement (the “double worsening” pattern), symptoms persisting beyond 10 days without any improvement, severe symptoms from onset (high fever above 39°C, unilateral facial pain and swelling), or unilateral maxillary toothache with fever. Only this category warrants antibiotic prescription — and even here, watchful waiting for 5–7 days before starting antibiotics is appropriate in mild-to-moderate cases, as approximately 47% of bacterial sinusitis resolves spontaneously.
Subacute sinusitis persists for 4–12 weeks and represents the transitional phase between acute and chronic infection — often requiring more aggressive investigation to identify contributing factors (allergy, structural issues, immune compromise).
Chronic sinusitis (CRS) is defined as symptoms persisting for 12 weeks or longer despite attempted treatment. It affects approximately 15% of the population in India’s urban centres and is one of the most significant contributors to reduced quality of life and healthcare costs. Chronic sinusitis is not simply prolonged acute sinusitis — it represents a distinct pathophysiological state characterised by persistent mucosal inflammation, disrupted mucociliary clearance, and often a dysbiotic sinus microbiome. Its management requires systematic identification of driving factors: allergic sensitisation (present in 50–60% of CRS patients), structural abnormalities (deviated septum, nasal polyps, concha bullosa), immune dysfunction, aspirin sensitivity (NSAID-exacerbated respiratory disease), or in a smaller proportion, fungal involvement.
Allergic fungal sinusitis is a specific and often misdiagnosed form more prevalent in warm, humid climates — including much of India — characterised by a hypersensitivity response to fungal antigens within the sinuses. It is associated with nasal polyps, thick eosinophilic mucin (sometimes called “peanut butter” mucus for its thick, cheesy consistency), and a history of atopy. It does not respond to antibiotics and requires antifungal management and often surgery.
India-Specific Sinusitis Triggers — Why Sinusitis Is Particularly Prevalent in Indian Urban Environments
India’s urban environments create a specific combination of sinusitis triggers that makes the condition disproportionately prevalent and difficult to manage compared to temperate Western environments. Understanding these India-specific factors is essential for effective prevention and management.
Air pollution is the dominant environmental sinusitis driver in Indian cities — with particulate matter (PM2.5), nitrogen dioxide, sulphur dioxide, ozone, and volatile organic compounds from vehicle exhaust, industrial emissions, and construction dust constantly present in concentrations that the WHO and Indian CPCB classify as hazardous for significant portions of the year in Delhi, Mumbai, Kolkata, and many other metros. These pollutants damage ciliary function (reducing mucociliary clearance efficiency), increase mucosal inflammation directly, and alter the sinus microbiome toward pro-inflammatory dysbiosis — creating exactly the conditions that predispose to recurrent sinusitis.
Rapid temperature changes — between air-conditioned indoor environments and outdoor heat in Indian summers — cause abrupt changes in nasal mucosal blood flow and secretion patterns that trigger rhinitis and sinus congestion in susceptible individuals. The prevalence of air conditioning in urban India has been identified as a contributing factor to the increasing incidence of both rhinitis and sinusitis.
Dust and seasonal allergens — including specific regional pollens, dust mites (whose populations thrive in India’s humid conditions), and indoor moulds in older buildings — drive the allergic rhinosinusitis that underlies a significant proportion of both acute and chronic sinusitis in India. The prevalence of allergic rhinitis in India is estimated at 20–30% of the urban population — and allergic rhinitis is the strongest single risk factor for chronic sinusitis.
Symptoms of Sinusitis — What Each Sign Tells You
Understanding what each sinusitis symptom represents physiologically helps you assess severity and choose appropriate management.
Nasal congestion and obstruction results from mucosal oedema — the vasodilation and plasma leakage that inflammation causes in the highly vascular nasal turbinates. It impairs breathing, reduces olfaction, and blocks sinus ostia — the fundamental pathophysiological event of sinusitis. Congestion that alternates between nostrils throughout the day is often normal physiological cycling (the nasal cycle, a phenomenon of alternating congestion and decongestion between left and right nasal passages that occurs every 1–4 hours); persistent bilateral blockage represents pathological oedema.
Facial pain and pressure characteristically localises to the affected sinus: maxillary sinusitis produces cheek pain (often described as toothache in upper teeth) that worsens on bending forward; frontal sinusitis produces forehead pain worse in the morning; ethmoid sinusitis produces pain between and behind the eyes; sphenoid sinusitis (the rarest) produces deep retro-orbital or vertex head pain. The “worsening on bending forward” characteristic is almost pathognomonic of sinusitis and distinguishes sinus headache from tension-type or migraine headache.
Nasal discharge character provides important diagnostic information: clear watery discharge suggests viral or allergic aetiology; thick yellow-green discharge indicates neutrophilic inflammation (consistent with bacterial infection or late viral) but is NOT specific for bacterial infection alone — viral sinusitis also produces coloured discharge. The common assumption that “green mucus = bacterial infection requiring antibiotics” is not supported by evidence: mucus colour reflects neutrophil activity and myeloperoxidase content, not bacterial versus viral aetiology.
Post-nasal drip — the sensation of mucus flowing down the back of the throat — causes the chronic throat-clearing, cough (particularly a morning cough and a cough on lying down), and voice changes that are common sinusitis complaints. In chronic sinusitis, post-nasal drip is often the dominant symptom more prominent than frank nasal congestion.
Hyposmia or anosmia (reduced or absent sense of smell) results from mucosal oedema blocking the olfactory cleft — the narrow passage at the roof of the nasal cavity where olfactory neurons are concentrated. Recovery of smell with improvement of congestion distinguishes conductive anosmia (from obstruction) from sensorineural anosmia (from neuronal damage, as in post-COVID anosmia). Persistent anosmia after nasal congestion resolves warrants further investigation.
12 Powerful Home Remedies for Sinusitis — With Full Mechanisms
1. Nasal Saline Irrigation — The Most Evidence-Backed Sinusitis Remedy
Nasal saline irrigation — rinsing the nasal passages with salt water using a neti pot, squeeze bottle, or bulb syringe — is the single most evidence-backed non-pharmacological sinusitis treatment available. Multiple systematic reviews and meta-analyses confirm its efficacy, and it is recommended as first-line management by ENT guidelines globally for both acute and chronic sinusitis.
Its mechanisms are multiple: mechanical flushing removes mucus, allergens, pollutants, biofilm-forming bacteria, and inflammatory mediators from the nasal and sinus mucosa. Hypertonic saline (higher salt concentration than body fluids) additionally draws fluid out of oedematous nasal mucosa through osmosis, reducing congestion. And regular saline irrigation improves mucociliary clearance — the fundamental defence mechanism against sinusitis — by cleaning and hydrating the ciliated epithelium, allowing the cilia to beat more effectively and move mucus toward the ostia.
A Cochrane review found that saline nasal irrigation significantly improved symptom scores, quality of life, and mucociliary clearance in chronic sinusitis — and reduced the need for medication. A clinical trial in children found that twice-daily nasal saline irrigation reduced sinusitis episodes by 36% compared to controls over 6 months. The traditional Indian Jala Neti practice — a yogic nasal cleansing technique practised for millennia — is the same intervention that modern evidence-based ENT practice now formally recommends. Ayurveda’s prescience in this area is remarkable.
Preparation: Use sterile water (boiled and cooled, or distilled — never tap water directly, as tap water can contain Naegleria fowleri amoeba in some Indian municipal water systems). Dissolve one quarter teaspoon of non-iodised salt (pickling salt, not table salt which contains anti-caking agents) in 240ml of sterile water. The solution should taste similar to tears. Tilt your head sideways over a sink. Pour the solution into the upper nostril and allow it to flow out through the lower nostril. Gently blow the nose after irrigation. Repeat twice daily during acute sinusitis episodes, once daily for maintenance in chronic sinusitis.
2. Steam Inhalation — Mucosal Hydration and Mucociliary Support
Steam inhalation is one of the most universally used and physiologically rational home remedies for sinusitis — and its mechanisms, while straightforward, are clinically meaningful. Inhaling warm, humidified air moisturises and warms the nasal and sinus mucosa, liquefying thick viscous mucus to a more watery consistency that moves more easily toward the sinus ostia and can be expelled more effectively. It also reduces mucosal oedema temporarily through the vasodilatory effects of local warming, improving ostial patency and sinus drainage.
Research on steam inhalation for sinusitis shows modest but consistent symptomatic benefit — primarily through the humidity effect rather than the heat itself. The addition of eucalyptus oil (containing 1,8-cineole) enhances the effect: 1,8-cineole has documented mucolytic properties (reducing mucus viscosity), direct antimicrobial activity against the respiratory pathogens responsible for sinusitis (S. pneumoniae, H. influenzae), and anti-inflammatory effects on airway mucosa through inhibition of cytokine production. A randomised controlled trial published in Laryngoscope found that 1,8-cineole significantly reduced sinusitis symptoms compared to placebo — at doses achievable through steam inhalation with eucalyptus oil.
Practical method: Bring 500ml of water to a boil. Allow it to cool for 1–2 minutes (scalding steam can damage nasal mucosa). Add 3–5 drops of eucalyptus oil or a small handful of fresh tulsi leaves. Create a steam tent by draping a towel over your head and the bowl. Inhale slowly and deeply through the nose for 5–10 minutes. Perform 2–3 times daily during acute sinusitis. Do not use essential oils with young children under 2 years — eucalyptus oil can cause reflex laryngospasm in very young children.
3. Tulsi (Holy Basil) — Ayurveda’s Complete Respiratory Herb
Tulsi (Ocimum tenuiflorum) is the most revered medicinal herb in Indian tradition — and for sinusitis specifically, its combination of antimicrobial, anti-inflammatory, mucolytic, and immunomodulatory properties makes it one of the most comprehensively appropriate single herbs for managing the condition.
Eugenol in tulsi has documented broad-spectrum antimicrobial activity including against the common sinusitis pathogens S. pneumoniae and H. influenzae. Ursolic acid and rosmarinic acid have direct anti-inflammatory effects on respiratory mucosa through NF-κB inhibition and prostaglandin synthesis reduction — addressing the mucosal oedema that drives ostial obstruction. And the immunomodulatory effects of tulsi (increasing NK cell and T-helper cell activity, as documented in double-blind clinical trials discussed in our immune system guide) support the body’s own capacity to resolve the infection.
The traditional Indian practice of chewing 4–5 fresh tulsi leaves each morning is an immune-supportive and respiratory-protective practice with a specific Ayurvedic rationale — the Shleshma-reducing (mucus-reducing) and Kapha-balancing properties of tulsi that Ayurveda describes for Pratishyaya correspond to its mucolytic and anti-inflammatory mechanisms. Tulsi tea — fresh or dried leaves steeped in boiling water for 5 minutes — concentrated with ginger and honey provides a triple combination of antimicrobial and anti-inflammatory support for acute sinusitis management.
4. Ginger-Turmeric Steam and Tea — The Anti-Inflammatory Power Combination
Ginger and turmeric represent the most important anti-inflammatory spice pairing in Ayurvedic respiratory medicine — and both have documented mechanisms relevant to sinusitis management that complement each other through different inflammatory pathway targets.
Ginger’s gingerols and shogaols inhibit prostaglandin synthesis (reducing mucosal vasodilation and oedema) and have direct antiviral activity against rhinovirus — the primary cause of viral sinusitis. Fresh ginger steeped in boiling water and inhaled as steam also delivers gingerol vapour directly to the sinus mucosa, providing localised anti-inflammatory effect at the site of pathology. As a tea (1-inch fresh ginger, steeped 10 minutes in 300ml water, with honey and lemon), ginger provides the systemic anti-inflammatory and mucolytic benefits documented in research — and the warmth of the liquid itself supports mucosal hydration and mucus liquefaction.
Turmeric’s curcumin specifically inhibits MUC5B and MUC5AC — the mucin genes responsible for the thick, gel-forming mucus produced in sinusitis — reducing mucus viscosity and improving clearance. It also reduces eosinophilic inflammation — the allergic inflammatory pattern that drives both allergic rhinosinusitis and nasal polyp formation. As covered in our anti-inflammatory foods guide, curcumin requires fat and piperine for optimal absorption — golden milk (haldi doodh with black pepper and ghee) is the most appropriate therapeutic preparation for addressing the systemic inflammation driving chronic sinusitis, not merely adding turmeric powder to water.
5. Neti Pot With Herbal Saline — The Enhanced Irrigation
The basic saline irrigation described above can be enhanced with specific herbal additions that provide therapeutic benefits beyond simple mechanical flushing. The most evidence-supported herbal additions to nasal saline are: a drop of pure neem extract (diluted — neem’s nimbidin has documented antimicrobial activity against sinus pathogens), and a small amount of xylitol (a natural sugar alcohol that disrupts bacterial biofilm formation on sinus mucosa — biofilm disruption being one of the key mechanisms in chronic bacterial sinusitis treatment).
The traditional Ayurvedic Nasya therapy — the application of medicated oils or herbal preparations through the nasal route — represents a sophisticated topical drug delivery system that predates modern nasal spray technology by thousands of years. Anu Taila — a classical Ayurvedic nasya oil containing sesame oil with herbs including Bala, Brahmi, and several others — is the most documented Ayurvedic nasya for chronic sinusitis. A clinical study published in the International Journal of Ayurveda Research found Anu Taila Nasya significantly improved subjective symptoms of chronic sinusitis over 4 weeks of daily morning use — providing preliminary clinical evidence for the therapeutic rationale of medicated nasya in chronic sinusitis management.
6. Ajwain (Carom Seeds) Steam — India’s Decongestant Herb
Ajwain (Trachyspermum ammi) — carom seeds, one of the most potent carminative and respiratory herbs in Indian Ayurvedic practice — contains thymol as its primary bioactive compound, a monoterpene with documented mucolytic, bronchodilatory, and antimicrobial properties that make it particularly valuable for sinusitis and upper respiratory congestion.
Thymol’s mechanism for sinusitis relief is multi-dimensional: it directly reduces mucus viscosity through mucolytic action on mucin glycoprotein cross-links, it produces bronchodilation through smooth muscle relaxation that extends to the upper respiratory tract, and it has antimicrobial activity against both S. pneumoniae and H. influenzae — the primary bacterial sinusitis pathogens. When ajwain seeds are heated or crushed, they release thymol vapour — making ajwain steam inhalation a delivery method for thymol directly to the sinus and nasal mucosa.
Traditional preparation: Heat a teaspoon of ajwain seeds in a dry pan until they release their aroma. Inhale the steam directly from the pan (held at safe distance) or wrap the heated seeds in a thin cloth and hold near the nose for inhalation. Alternatively, add a tablespoon of ajwain seeds to boiling water, create a steam tent, and inhale for 5–7 minutes. The traditional Indian practice of tying ajwain in a cloth and sniffing it for congestion is a delivery mechanism with genuine pharmacological rationale.
7. Garlic — Antimicrobial and Mucolytic Support
Garlic’s allicin — the bioactive compound produced when garlic is crushed or chopped, triggering the enzymatic conversion of alliin by alliinase — has broad-spectrum antimicrobial activity against the primary bacterial pathogens of sinusitis, documented mucolytic effects that reduce mucus viscosity, and direct anti-inflammatory activity through NF-κB inhibition and prostaglandin synthesis reduction.
Research on garlic for respiratory infections is extensive: a randomised controlled trial found garlic supplementation reduced cold incidence by 63% and reduced cold duration by 70% compared to placebo — effects mediated through both the direct antimicrobial activity of allicin and garlic’s immunomodulatory effects on NK cell and macrophage function. While this trial addressed cold prevention rather than sinusitis treatment specifically, the mechanisms are directly relevant — viral respiratory infections are the primary trigger for acute sinusitis.
For sinusitis specifically, fresh garlic consumed raw (2–3 cloves daily, crushed and allowed to sit for 10 minutes before consumption to maximise allicin formation) provides therapeutic allicin concentrations that support both viral and bacterial sinusitis resolution. Garlic’s allicin also reaches the respiratory mucosa through the breath after consumption — the same mechanism that makes breath smell of garlic delivers antimicrobial allicin vapour to the nasal passages and sinuses. The complete evidence for garlic as an essential herb is covered in our essential herbs for winter immunity guide.
8. Apple Cider Vinegar and Honey — Antimicrobial and pH-Modulating Support
Apple cider vinegar (ACV) with honey is one of the most widely used traditional remedies for sinusitis — and while it lacks direct clinical trial evidence specific to sinusitis, its mechanisms provide a biologically plausible rationale. Raw apple cider vinegar contains acetic acid (demonstrated antimicrobial activity through disruption of bacterial cell membranes), malic acid, and beneficial enzymes — and when diluted in warm water, it may modestly thin mucus secretions through its acidic pH, which reduces mucin crosslinking and decreases viscosity.
Raw honey — particularly dark honey varieties like buckwheat honey — has the strongest evidence for respiratory antimicrobial effects, primarily through its hydrogen peroxide generation, osmotic dehydration of bacteria, and methylglyoxal content in Manuka honey. Research has documented raw honey’s activity against biofilm-forming H. influenzae — one of the primary bacterial sinusitis pathogens — at concentrations achievable in the upper respiratory tract from ingested honey. The combination of ACV and honey in warm water provides a warm liquid that supports mucosal hydration alongside these antimicrobial compounds.
9. Eucalyptus and Peppermint — Direct Mucolytic and Decongestant Action
Eucalyptus oil (containing primarily 1,8-cineole / eucalyptol) and peppermint oil (containing menthol and menthone) are the most clinically studied essential oils for respiratory conditions, with documented mechanisms that are particularly relevant to sinusitis management.
1,8-cineole has the strongest evidence of any single aromatic compound for sinusitis — the randomised controlled trial in Laryngoscope mentioned earlier found it significantly reduced sinusitis symptom scores, and research published in the Journal of Laryngology and Otology found oral 1,8-cineole capsules (EfacoR) significantly outperformed placebo for acute sinusitis treatment. The mechanism includes: mucolytic effects (reducing mucus viscosity and improving clearance), direct antimicrobial activity against the primary sinusitis pathogens, and anti-inflammatory effects through inhibition of inflammatory cytokine production in airway epithelial cells.
Menthol from peppermint activates cold-sensitive TRPM8 receptors in the nasal mucosa, producing the subjective sensation of improved airflow even when objective nasal resistance is unchanged — important for comfort but not truly decongestant. More significantly, menthol has cilia-activating effects that improve mucociliary clearance velocity, directly addressing the fundamental pathophysiological defect of sinusitis. Diluted peppermint oil applied externally to the temples and forehead also provides the menthol-receptor activation that reduces the perception of sinus pressure and facial pain.
10. Warm Liquids and Adequate Hydration — The Underrated Foundation of Recovery
The connection between adequate hydration and sinusitis recovery is mechanistically direct: mucus viscosity is inversely proportional to the hydration state of the mucous layer. Dehydrated mucus is thick, poorly mobile, and difficult for cilia to transport toward the sinus ostia — precisely the conditions that lead to stagnation, bacterial growth, and prolonged symptoms. Well-hydrated mucus is more watery, more effectively moved by ciliary action, and drained more efficiently through the ostia.
As covered in our hydration guide, 30–35ml per kg of body weight of fluids daily is the appropriate target — increased during acute infection when fever and increased respiratory rate accelerate fluid losses. Beyond plain water, specific hot liquids have additional benefits: hot soups (particularly the traditional Indian yakhni shorba or chicken soup — whose scientific rationale includes mild anti-inflammatory cytokine reduction documented in a clinical study, and cysteine from the broth that thins mucus secretions), hot herbal teas (tulsi, ginger, peppermint — delivering therapeutic compounds through the vapour and the liquid simultaneously), and warm water with lemon (citric acid modestly reduces mucus viscosity).
11. Nasya (Medicated Oil Application) — Ayurveda’s Direct Sinus Therapy
Nasya — the Ayurvedic practice of applying small quantities of medicated oil through the nasal passages — is one of the five Panchakarma cleansing procedures and the primary Ayurvedic treatment for disorders of the head, neck, and sinuses. In the context of sinusitis, specifically Pratimarsha Nasya (daily preventive nasya using small quantities of oil) is the most clinically relevant application.
The physiological rationale is well-supported: applying a thin film of sesame oil or ghee to the nasal mucosa provides a physical barrier that reduces adherence of allergens, pollutants, and pathogens to the mucosal surface — directly reducing the trigger exposure that initiates sinusitis episodes. It also prevents the mucosal desiccation that occurs in air-conditioned environments and during winter, maintaining the mucosal hydration and ciliary function that are fundamental to sinus health. A small amount of warm sesame oil or ghee applied to each nostril with the little finger — the traditional nasya practice — creates this protective film with no risk and significant preventive benefit.
For acute sinusitis, classical Ayurveda prescribes more intensive Nasya using medicated oils including Anu Taila — with the clinical evidence referenced above suggesting genuine therapeutic benefit in chronic sinusitis from daily medicated nasya application. This practice is most beneficial when performed in the morning after nasal saline irrigation has cleared the mucosa of stagnant secretions.
12. Spiced Indian Kadha — The Traditional Immune and Respiratory Support Preparation
Kadha — the traditional Indian medicinal decoction prepared by simmering multiple herbs and spices in water — is one of the most practically effective and most culturally integrated natural remedies for sinusitis and upper respiratory infections. The traditional composition varies by region and family tradition, but the most evidence-supported sinusitis-specific kadha combines: tulsi (antimicrobial and immunomodulatory), ginger (anti-inflammatory and mucolytic), black pepper (piperine — improves absorption of other bioactive compounds and has direct antimicrobial activity), cinnamon (anti-inflammatory through cinnamaldehyde), clove (eugenol — antimicrobial and analgesic), and honey added after cooling (preserving enzyme activity and antimicrobial properties).
The evidence base for kadha as a preparation specifically for sinusitis includes the documented activities of each ingredient through multiple mechanisms targeting different aspects of the sinusitis pathophysiology: the viral trigger, the inflammatory mucosal response, the viscous mucus accumulation, and the secondary bacterial risk. During the COVID-19 pandemic, the Indian Ministry of AYUSH formally recommended a specific kadha formulation (tulsi, dalchini, kalimirch, saunth, munakka) — and while COVID-19 is distinct from sinusitis, the immune-supportive and upper respiratory anti-inflammatory rationale is directly applicable. The comprehensive herb profile supporting these ingredients is covered in our articles on essential herbs for winter immunity and the natural immune system guide.
Kadha preparation: Combine 2 cups water, 8–10 fresh tulsi leaves, 1-inch sliced fresh ginger, 4–5 black peppercorns, 1 small cinnamon stick, 2–3 cloves, and optionally a pinch of cardamom. Bring to a boil and simmer for 10–15 minutes until the liquid reduces by about one-third. Strain. Add 1 teaspoon of raw honey once the liquid is warm (not boiling). Drink 1–2 cups daily during acute upper respiratory illness or sinusitis episodes.
Conventional Medical Treatments — When and Why
Understanding the appropriate role of conventional medical treatments for sinusitis prevents both under-treatment (inadequate management of bacterial sinusitis) and over-treatment (unnecessary antibiotics for viral sinusitis, the most common medical sinusitis management error globally).
Intranasal corticosteroid sprays (fluticasone, budesonide, mometasone) are the most effective pharmacological treatment for chronic sinusitis and allergic rhinosinusitis — reducing mucosal oedema through glucocorticoid receptor-mediated suppression of the inflammatory cascade that drives persistent obstruction. Unlike oral steroids, intranasal administration provides topical mucosal effect with minimal systemic absorption, making them safe for long-term daily use. Multiple systematic reviews confirm their efficacy for both acute and chronic sinusitis symptom reduction. They are the single most important pharmacological intervention for chronic sinusitis and should be the first medical treatment considered before antibiotics.
Antibiotics are appropriate specifically for acute bacterial sinusitis — characterised by the clinical features described above (double worsening pattern, symptoms beyond 10 days, severe unilateral facial pain and fever). Even in confirmed bacterial sinusitis, watchful waiting for 5–7 days before prescribing is supported by evidence showing that 47% of bacterial sinusitis resolves spontaneously. Amoxicillin-clavulanate is the first-line antibiotic for bacterial sinusitis in India where beta-lactamase resistance is prevalent. Fluoroquinolones should be reserved for cases with penicillin allergy or previous treatment failure — not as first-line therapy. Antibiotic resistance is a growing concern in sinusitis management globally, and inappropriate antibiotic prescribing for viral sinusitis is a major contributor.
Antihistamines are appropriate for allergic rhinosinusitis where allergen sensitisation is confirmed — second-generation non-sedating antihistamines (cetirizine, loratadine, fexofenadine) are preferred for daytime use. They address the allergic inflammatory trigger but do not treat the mucosal oedema of non-allergic sinusitis.
Functional endoscopic sinus surgery (FESS) is indicated for chronic sinusitis that has not responded to adequate medical management (typically at least 12 weeks of nasal steroid spray, saline irrigation, and treatment of any identified allergic triggers), or for structural abnormalities (deviated septum with symptomatic obstruction, nasal polyps causing significant obstruction, or anatomical variants blocking the ostiomeatal complex). Modern FESS is a minimally invasive endoscopic procedure that widens the sinus ostia and removes obstructing tissue — restoring the drainage that is the fundamental defect in chronic sinusitis.
Sinusitis: Myth vs. Fact
| ❌ The Myth | ✅ The Truth |
|---|---|
| Green or yellow mucus means you need antibiotics | Mucus colour reflects neutrophil activity and the presence of myeloperoxidase — not bacterial versus viral aetiology. Clear mucus, white mucus, yellow mucus, and green mucus can all occur in both viral and bacterial sinusitis. The colour alone is not an indication for antibiotics. Clinical features (symptom duration, fever pattern, severity, double worsening) are the relevant criteria — not mucus colour. |
| Chronic sinusitis can always be cured with a course of antibiotics | The majority of chronic sinusitis is driven by inflammation — not active bacterial infection. Long-term antibiotic courses are not the appropriate treatment for most chronic sinusitis. The primary interventions are nasal steroid sprays, saline irrigation, allergy management (if relevant), and in refractory cases, surgery. Inappropriate antibiotic use contributes to antibiotic resistance without improving chronic sinusitis outcomes. |
| Sinusitis is purely an infection — it has nothing to do with allergies or diet | Allergic rhinosinusitis — driven by IgE-mediated hypersensitivity to airborne allergens — is the primary driver of chronic sinusitis in 50–60% of affected patients. Diet influences sinusitis through inflammatory and immune mechanisms: dairy’s potential to increase mucus production in some individuals, anti-inflammatory foods’ effects on mucosal inflammation, and gut microbiome health’s influence on mucosal immune function all have evidence-supported connections to sinusitis frequency and severity. |
| Neti pot (nasal irrigation) is dangerous for regular use | Nasal saline irrigation is recommended by ENT guidelines for both acute and chronic sinusitis management. When performed correctly with sterile (boiled or distilled) water and appropriate saline concentration, it is safe for daily long-term use. The rare reported cases of amoebic meningoencephalitis from neti pot use have all involved tap water or inadequately treated water — never sterile saline preparation. The neti pot itself is completely safe when used with properly prepared sterile saline. |
| Air conditioning helps sinusitis by keeping the environment clean | Air conditioning without regular filter maintenance can worsen sinusitis by circulating allergens, mould spores, and bacteria from dirty filters, and by dramatically reducing indoor humidity — drying the nasal mucosa and impairing mucociliary clearance. Clean, regularly maintained air conditioning with humidification support is neutral to beneficial; dirty air conditioning with low humidity is a significant sinusitis trigger in Indian office and home environments. |
| Surgery is the only option for chronic sinusitis | Surgery (FESS) is indicated for chronic sinusitis refractory to adequate medical management — not as a first-line or early treatment. Most chronic sinusitis improves significantly with consistently applied nasal steroid sprays, regular saline irrigation, allergy identification and management, and environmental modification. Surgery is reserved for cases where 12+ weeks of appropriate medical management has failed or where structural abnormalities (significant polyps, deviated septum) are driving recurrence. |
When to See a Doctor — Red Flags That Require Urgent Attention
While most acute sinusitis resolves with the home remedies and supportive care in this guide, certain symptoms indicate serious complications that require immediate or urgent medical evaluation.
Seek urgent medical care (same day or emergency department) for: high fever (above 39°C) with severe headache or stiff neck (meningitis must be excluded); swelling or redness around one or both eyes (orbital cellulitis or orbital abscess — a serious complication of ethmoid sinusitis); sudden severe headache described as “the worst headache of my life” (subarachnoid haemorrhage must be excluded); confusion or altered consciousness; frontal swelling or oedema (Pott’s puffy tumour — a rare complication of frontal sinusitis); or any visual changes including double vision or reduced visual acuity.
See a doctor within 2–3 days for: symptoms not improving after 10 days, or symptoms that initially improved then significantly worsened (the “double worsening” pattern suggesting bacterial superinfection); fever that develops after several days of worsening rather than improving symptoms; multiple episodes of sinusitis in a single year (more than 3 episodes per year suggests underlying allergic, anatomical, or immune factor requiring investigation); or sinusitis in a diabetic patient, immunocompromised individual, or someone on corticosteroid therapy (these populations are at higher risk for complications including fungal sinusitis).
Preventing Sinusitis Recurrence — The Long-Term Strategy
For people with recurrent or chronic sinusitis, prevention is as important as treatment. The most evidence-backed preventive strategies include: addressing allergic triggers through allergen testing and targeted avoidance or immunotherapy (the only intervention that modifies the underlying allergic disease rather than managing symptoms); daily nasal saline irrigation to maintain mucociliary clearance; daily Pratimarsha Nasya with sesame oil or ghee to protect the nasal mucosa from environmental triggers; addressing indoor air quality including regular air conditioning filter maintenance and appropriate humidity levels (40–60% relative humidity is optimal for mucociliary function); supporting immunity through the comprehensive framework in our natural immune system guide; and reducing the chronic inflammation that perpetuates mucosal oedema through the anti-inflammatory dietary approach in our anti-inflammatory foods guide.
Related Articles From HerbeeLife
📖 Natural Ways to Boost Your Immune System: 12 Science-Backed Strategies
📖 Essential Herbs for Winter Immunity: 10 Powerful Natural Remedies That Actually Work
📖 Anti-Inflammatory Foods: 12 Powerful Choices That Fight Disease From the Inside Out
📖 How to Improve Digestion Naturally: 12 Powerful Science-Backed Strategies
📖 Amla Benefits: Proven Immunity, Digestion and Whole-Body Health Backed by Science
📖 Ashwagandha for Stress and Anxiety: What Actually Happens in Your Body
📖 Holistic Health Benefits: 7 Life-Changing Reasons to Treat Your Whole Self
Frequently Asked Questions: Sinusitis Causes, Symptoms and Treatment
How do I know if my sinus infection is viral or bacterial?
The clinical distinction is challenging even for experienced clinicians because symptoms overlap substantially. Features suggesting bacterial rather than viral sinusitis include: symptoms persisting beyond 10 days without any improvement (most viral sinusitis begins improving by day 7–10); the “double worsening” pattern — initial improvement followed by significant deterioration after day 5–6; severe symptoms from the outset, particularly high fever above 39°C with unilateral facial pain and tenderness; and unilateral maxillary toothache with fever. Even with these features, watchful waiting for 5–7 days before antibiotics is appropriate in mild-to-moderate cases, as bacterial sinusitis often resolves without treatment.
Is it safe to do neti pot (Jala Neti) every day?
Yes — daily nasal saline irrigation is recommended by ENT guidelines for chronic sinusitis management and is safe for long-term daily use when performed with properly prepared sterile (boiled and cooled or distilled) water and appropriate saline concentration. Never use tap water directly — the rare serious complications from neti pot use have all involved non-sterile tap water. The correct technique — head tilted sideways, gentle low-pressure flow — is important; forceful high-pressure irrigation can push contaminated water into the middle ear through the Eustachian tube. Proper preparation and technique make this one of the safest and most effective daily sinusitis management practices available.
Can diet affect sinusitis severity?
Yes, through multiple mechanisms. Dairy consumption increases mucus production in some (not all) individuals by stimulating goblet cells in the respiratory mucosa — reducing dairy during acute sinusitis episodes may reduce mucus burden in dairy-sensitive individuals. A diet high in refined carbohydrates and processed foods promotes systemic inflammation that can worsen sinus mucosal inflammation. Anti-inflammatory dietary patterns (turmeric, ginger, omega-3-rich foods, diverse plant foods) reduce the inflammatory substrate that drives persistent mucosal oedema. And gut microbiome health — supported by the dietary approach in our digestion guide — directly influences mucosal immune function in the airways through the gut-airway immune axis.
What is the Ayurvedic view of sinusitis?
In Ayurveda, sinusitis — classified as Pratishyaya — is understood primarily as a Kapha and Vata disorder, with accumulation of excess Kapha (mucus, heaviness, congestion) combined with Vata-driven dryness in some manifestations. The primary Ayurvedic treatments are Nasya (medicated nasal oil application), Neti (nasal cleansing with saline — the same practice ENT medicine now recommends), steam inhalation with Kapha-reducing herbs (ginger, ajwain, eucalyptus, tulsi), and internal herbs that reduce Kapha and support Agni (digestive fire and mucosal immunity). The Ayurvedic approach also emphasises dietary Kapha reduction: avoiding cold foods and beverages, excessive dairy, and sweet-heavy foods during active sinusitis episodes; favouring warm, light, spiced foods that support mucosal dryness and drainage.
When do I need surgery for sinusitis?
Functional endoscopic sinus surgery (FESS) is indicated when chronic sinusitis has failed to respond to at least 12 weeks of adequate medical management (consistent nasal steroid spray use, regular saline irrigation, treatment of identified allergic triggers), particularly when CT scan confirms significant mucosal thickening, polyps, or anatomical obstruction. It is also indicated for: nasal polyps causing significant nasal obstruction or symptoms despite medical treatment; confirmed allergic fungal sinusitis (which often requires surgical removal of fungal debris); anatomical variants (such as a significantly deviated septum blocking the ostiomeatal complex) that are clearly driving recurrent infection; and any sinusitis with orbital or intracranial complications. Surgery is not a first-line treatment but is highly effective when correctly indicated.
Sources and References
1. Fokkens WJ et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2016 (EPOS 2016). Rhinology, 2016.
2. Pynnonen MA et al. Clinical Practice Guideline: Adult Sinusitis Executive Summary. Otolaryngology-Head and Neck Surgery, 2015.
3. Rabago D, Zgierska A. Saline nasal irrigation for upper respiratory conditions. American Family Physician, 2009.
4. Juergens UR et al. Anti-inflammatory activity of 1.8-cineol (eucalyptol) in bronchial asthma. Respiratory Medicine, 2003.
5. Zalmanovici Trestioreanu A, Yaphe J. Intranasal steroids for acute sinusitis. Cochrane Database of Systematic Reviews, 2013.
6. Lemiengre MB et al. Antibiotics for clinically diagnosed acute rhinosinusitis in adults. Cochrane Database of Systematic Reviews, 2012.
7. Kumar A et al. Clinical evaluation of Anu taila Nasya in the management of Dushta Pratishyaya. International Journal of Ayurveda Research, 2017.
Follow HerbeeLife
🌿 Stay connected for more evidence-based health guidance, Ayurvedic wisdom, and Indian wellness content:
📸 Instagram | 📌 Pinterest | 👥 Facebook | 🐦 X (Twitter)
Final Thoughts: Most Sinusitis Resolves — But What You Do in the Meantime Matters Enormously
The most important single insight from this entire guide is that 98% of acute sinusitis is viral — and antibiotics do nothing for viruses. The most important interventions for the vast majority of sinusitis episodes are the home remedies and natural strategies in this guide: nasal saline irrigation to restore the fundamental drainage mechanism of the sinuses, steam inhalation to hydrate and liquefy mucus, tulsi-ginger-ajwain to reduce mucosal inflammation and provide antimicrobial support, and adequate hydration to maintain mucus fluidity.
And beyond the acute episode, the most important sinusitis strategy is prevention: daily Nasya to protect the nasal mucosa, regular Jala Neti during high-exposure periods, addressing allergic triggers systematically, and maintaining the immune resilience that reduces the frequency and severity of the viral upper respiratory infections that initiate most sinusitis episodes.
India’s Ayurvedic tradition has practised every one of these strategies for thousands of years. Modern ENT medicine has confirmed the mechanisms. Your grandmother’s kadha was not superstition. It was pharmacology.
⚠️ Medical Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. Sinusitis, particularly with high fever, orbital swelling, severe headache, or symptoms beyond 10 days, requires professional medical evaluation. Never delay seeking medical care because of information in this article. Read full disclaimer →
💬 Which of these 12 home remedies have you tried for sinusitis — and which traditional Indian remedy from your family has worked best? Share in the comments. And if you struggle with chronic sinusitis in India’s polluted cities, we especially want to hear your experience and what has helped most.

