
We go from the biology of how cholesterol causes harm, to the specific LDL-reduction percentages achievable with each natural strategy, to the India-specific foods and herbs (amla, methi, guggulu) that have genuine clinical evidence, to the honest discussion of when natural management is sufficient and when statins become essential. Natural ways to lower cholesterol are powerful — and powerfully enhanced when you understand the mechanisms.
Understanding Cholesterol — The Biology That Explains Why What You Eat Matters
Cholesterol is not inherently harmful — it is a necessary component of every cell membrane in the body, the building block of steroid hormones (including testosterone, oestrogen, and cortisol), bile acids (needed for fat digestion), and Vitamin D. The problem is not cholesterol itself — it is where cholesterol accumulates and in what form.
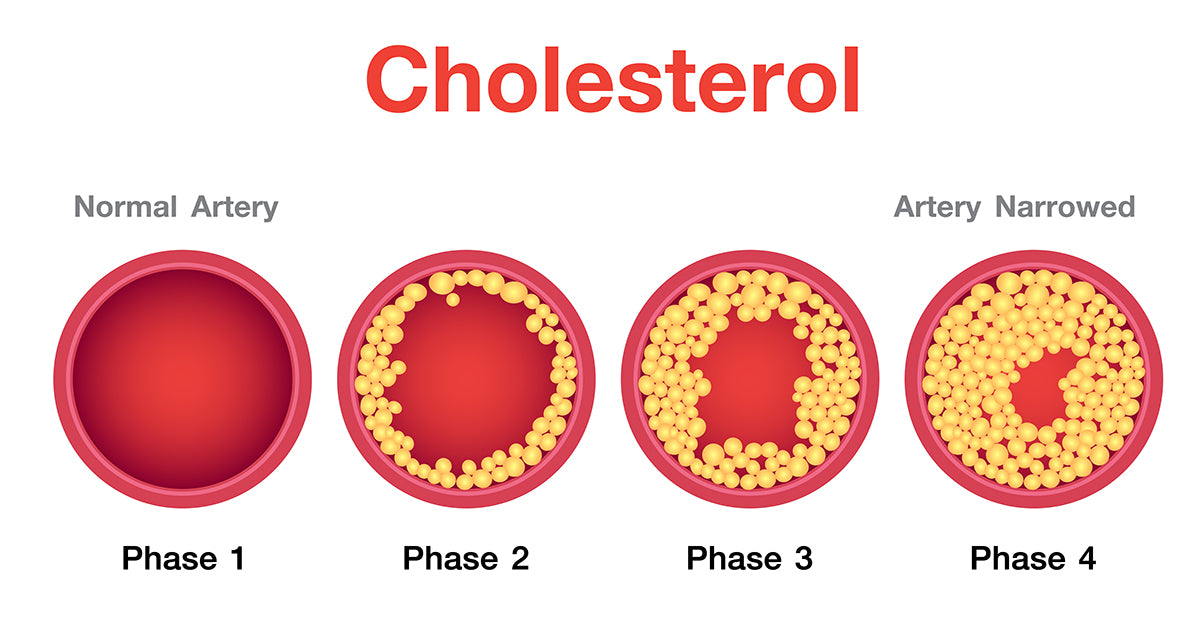
LDL (Low-Density Lipoprotein) — “Bad” Cholesterol: LDL particles transport cholesterol from the liver to peripheral tissues. When LDL is elevated — particularly small, dense LDL particles — cholesterol deposits in arterial walls, triggering oxidation and macrophage infiltration that produces atherosclerotic plaques. Target: <100 mg/dL for most adults; <70 mg/dL with existing cardiovascular disease. Reducing LDL is the primary focus of cholesterol management.
HDL (High-Density Lipoprotein) — “Good” Cholesterol: HDL particles transport cholesterol from peripheral tissues and arterial walls back to the liver for disposal — “reverse cholesterol transport.” Higher HDL is cardioprotective. Target: >40 mg/dL (men), >50 mg/dL (women); >60 mg/dL is independently protective. Indian adults typically have lower HDL than Western populations — making HDL-raising strategies particularly important.
Triglycerides: Blood fats derived from dietary carbohydrates and fat. Elevated triglycerides (>150 mg/dL) independently increase cardiovascular risk — particularly in South Asians where high triglycerides combined with low HDL (the “atherogenic dyslipidaemia” pattern) is extremely common. Reducing refined carbohydrates and alcohol reduces triglycerides more effectively than reducing dietary fat.
Non-HDL Cholesterol: Total cholesterol minus HDL — captures LDL + VLDL + IDL particles that all contribute to atherosclerosis. Increasingly preferred over LDL alone as a risk predictor, particularly in Indians with high triglycerides. Target: <130 mg/dL for most; <100 mg/dL with existing cardiovascular disease.
Lp(a) — Lipoprotein(a): An LDL particle with an additional apolipoprotein(a) protein attached. Elevated Lp(a) is an independent major cardiovascular risk factor — not reduced by diet, exercise, or standard statins. More common in South Asians than in Western populations. Most Indians have never been tested. Request Lp(a) measurement if you have a family history of premature heart disease or if your LDL appears well-controlled but cardiovascular events still occur. Read more on the heart attack risk significance: Heart Attack Warning Signs: Never Ignore These
10 Science-Backed Natural Ways to Lower Cholesterol — With the Mechanisms and Numbers
Soluble fibre is the single most evidence-backed dietary intervention for LDL reduction. The mechanism is direct and well-characterised: soluble fibre (found in oats, barley, isabgol, dal, fruits, and vegetables) dissolves in the intestinal contents to form a viscous gel that physically traps bile acids and prevents their reabsorption. The liver must then use more cholesterol to produce new bile acids — drawing cholesterol from the blood. This forces the liver to upregulate LDL receptor expression, pulling more LDL from the circulation. The result: measurable LDL reduction with every gram of soluble fibre consumed consistently.
A 2014 meta-analysis of 67 randomised trials found that each additional 10g of daily soluble fibre reduced LDL by approximately 5%. The clinical benchmark: 5–10g of soluble fibre daily (achievable through 1 serving of oats + 1 serving of dal + 1 serving of fruit) produces a consistent 5–7% LDL reduction — modest per intervention, but compounding when combined with other dietary changes.
Best Indian sources: Isabgol/psyllium husk (highest soluble fibre concentration per gram — 7g soluble fibre per tablespoon), oats (4g per cup cooked), barley (6g per cup cooked), all varieties of dal (4–6g per cup cooked), apples (2g), guava (3g), and fenugreek seeds/methi (concentrated soluble fibre as galactomannan).
Plant sterols and stanols are structurally similar to cholesterol and compete with it for absorption in the intestinal wall through the same NPC1L1 transporter. Consuming 2g of plant sterols or stanols daily reduces LDL by 10–15% — the largest single dietary intervention effect on LDL available, exceeding soluble fibre, omega-3s, and most herbs individually. A 2003 meta-analysis of 41 trials confirmed this effect consistently across populations. Plant sterols are present in all plant foods — but in amounts far too small to produce this effect from regular diet alone. The therapeutic dose requires supplementation or fortified foods.
Indian sources of plant sterols (for regular dietary contribution): Til (sesame seeds) — one of the highest plant sterol concentrations in common Indian foods at 400mg/100g; pumpkin seeds (265mg/100g); flaxseed; rice bran oil (notable phytosterol content — one reason rice bran oil is often recommended for heart-healthy Indian cooking); mustard oil; and legumes. These provide meaningful but sub-therapeutic sterol doses — useful as dietary contributors alongside targeted supplementation if LDL reduction goals require the full 10–15% effect.
⚗️ 2g/day plant sterols: 10–15% LDL reduction | 41-trial meta-analysis confirmation | NPC1L1 transporter competition mechanismAmla is the Indian herb with the strongest clinical evidence for cholesterol reduction — and the mechanism is pharmacologically remarkable. A 2012 double-blind, randomised, placebo-controlled trial in the European Journal of Clinical Nutrition found that amla extract (500mg twice daily) significantly reduced total cholesterol by 16%, LDL by 24%, triglycerides by 27%, and atherogenic index — while significantly increasing HDL by 14%. This is a comprehensive, favourable lipid profile change that few dietary interventions achieve.
The mechanisms: amla’s emblicanin A and B tannins inhibit HMG-CoA reductase — the rate-limiting enzyme in the liver’s cholesterol synthesis pathway, the same enzyme targeted by statin medications. Amla’s chromium content improves insulin sensitivity, reducing the liver’s production of VLDL (the precursor to LDL). Vitamin C (600–900mg per fresh amla — the highest plant concentration) reduces LDL oxidation — preventing the modification of LDL into its more atherogenic oxidised form. The combination produces a statin-like LDL reduction with additional antioxidant protection that statins do not provide.
Methi seeds address multiple components of the Indian atherogenic lipid profile simultaneously. Galactomannan (the concentrated soluble fibre in methi) reduces cholesterol absorption through the same bile acid sequestration mechanism as isabgol — but methi also contains saponins (steroidal glycosides) that specifically inhibit cholesterol absorption and intestinal acyl-coenzyme A transferase (an enzyme required for cholesterol esterification and absorption). The combined effect: reduced dietary cholesterol absorption + bile acid sequestration + 4-hydroxyisoleucine-mediated improvement in insulin sensitivity (reducing hepatic VLDL production and thus triglycerides).
A 2009 meta-analysis of clinical trials found that fenugreek seed supplementation significantly reduced total cholesterol, LDL, and triglycerides while modestly increasing HDL. The triglyceride-reducing effect is particularly valuable for the Indian lipid profile — where elevated triglycerides combined with low HDL are the dominant cardiovascular risk pattern. Methi addresses this pattern directly.
Berberine (found in daruharidra/Indian barberry, Berberis aristata) is the natural compound with the most impressive clinical cholesterol-lowering evidence outside of dietary fibre and plant sterols. The mechanism is distinctive and does not replicate statins: berberine increases the expression of LDL receptors on liver cells through PCSK9 inhibition and AMPK activation — the liver produces more LDL receptors, which then pull more LDL from the circulation. This is the same LDL receptor upregulation mechanism that makes the revolutionary PCSK9 inhibitor drugs (evolocumab, alirocumab) so effective — but achieved through a natural AMPK pathway rather than a pharmaceutical antibody.
A 2004 landmark study in Nature Medicine demonstrated that berberine reduced LDL by 25%, triglycerides by 35%, and total cholesterol by 29% in hyperlipidaemic patients over 12 weeks. A 2012 meta-analysis of 11 randomised trials confirmed significant reductions in LDL, triglycerides, and total cholesterol comparable to low-dose statins for mild-moderate dyslipidaemia. Berberine also improves glucose metabolism (relevant to the insulin resistance underlying Indian atherogenic dyslipidaemia), reduces hepatic fat accumulation (which drives VLDL overproduction), and has direct anti-inflammatory effects on vascular endothelium.
Important: Berberine interacts with several medications including blood thinners, cyclosporin, and diabetes medications. If on any regular medications, discuss berberine supplementation with your physician. The typical supplemental dose is 500mg 2–3 times daily with meals.
⚗️ Nature Medicine 2004: LDL -25%, TG -35% | PCSK9-independent LDL receptor upregulation | 11-RCT meta-analysis confirmationDietary fat type — more than total fat quantity — is the most important dietary determinant of LDL cholesterol. Replacing saturated fat (ghee, coconut oil, vanaspati, fatty meat, full-fat dairy) with unsaturated fat (mustard oil, olive oil, rice bran oil, walnuts, flaxseed) produces reliable and significant LDL reduction. A comprehensive 2015 Cochrane review found that replacing saturated with unsaturated fat reduced cardiovascular events by 17% — with each percentage point of calories replaced from saturated to unsaturated fat reducing LDL by approximately 2 mg/dL.
Trans fats — produced by partial hydrogenation of vegetable oils (vanaspati, dalda, and many commercial bakery products) — are the most harmful dietary fat for the lipid profile: they simultaneously raise LDL and lower HDL, the worst possible combination. India remains a significant consumer of vanaspati and trans-fat-containing products. Reading ingredient labels for “partially hydrogenated” fat and eliminating products containing it produces an immediate LDL benefit.
The ghee question: Pure ghee (clarified butter) is predominantly saturated fat. In quantities used in traditional Indian cooking (1–2 teaspoons per day), the evidence for harm is not strong. In larger quantities or in the context of an already high saturated fat diet, ghee replacement with cold-pressed mustard oil or rice bran oil (both with better fatty acid profiles for Indian cardiovascular risk) is advisable. The traditional Ayurvedic use of ghee in small amounts as a cooking medium is not the cardiovascular problem — the large quantities used in restaurant cooking and festive food preparation are.
⚗️ Cochrane 2015: saturated→unsaturated fat replacement reduces CVD events 17% | Trans fats: raise LDL + lower HDL simultaneouslyOmega-3 fatty acids (EPA and DHA from oily fish; ALA from walnuts, flaxseed, and mustard oil) are the most effective natural intervention specifically for triglyceride reduction — addressing the triglyceride component of the Indian atherogenic profile. The mechanism: omega-3s reduce hepatic VLDL production (the precursor to LDL and the primary carrier of triglycerides in blood), increase VLDL clearance from circulation through lipoprotein lipase activation, and reduce de novo lipogenesis (the liver’s conversion of excess carbohydrates to fat). High-dose omega-3s (2–4g EPA+DHA daily) reduce triglycerides by 20–50% — a dose-dependent effect with clinical trial support across multiple populations.
For Indian vegetarians: ALA from walnuts (5–7 daily) and ground flaxseed (1 tablespoon daily in curd or roti) provides the substrate for EPA and DHA synthesis, though the conversion rate is low (5–10%). Algae-based omega-3 DHA+EPA supplements (400–1,000mg daily) are the most direct vegetarian option for therapeutic triglyceride reduction. Cooking with mustard oil (relatively high in ALA compared to refined oils) provides a meaningful daily contribution. The triglyceride-HDL ratio (a sensitive marker of insulin resistance and atherogenic risk in Indians) improves measurably with consistent omega-3 intake.
⚗️ High-dose omega-3: 20–50% triglyceride reduction | Reduced hepatic VLDL production + lipoprotein lipase activation | TG:HDL ratio improvementGuggulu (Commiphora mukul resin, also called guggul) is the primary Ayurvedic herb historically used for cholesterol and metabolic management — and it has genuine pharmacological mechanisms supporting its traditional use. The active compounds guggulsterones (Z and E isomers) act as antagonists of the farnesoid X receptor (FXR) — a bile acid receptor that normally suppresses LDL receptor expression in the liver. By blocking FXR, guggulsterones maintain LDL receptor expression and enhance LDL clearance from the blood. They also modestly inhibit thyroid peroxidase, slightly increasing thyroid activity (which increases LDL receptor expression and cholesterol clearance).
Multiple Indian clinical trials (predominantly from the 1980s–2000s) showed significant LDL and triglyceride reduction with guggulu. However, a 2003 rigorous double-blind, placebo-controlled JAMA study found no significant LDL reduction — and mild LDL increase in some participants. The discrepancy may reflect differences in guggulsterone content between preparations, bioavailability issues, and study design differences. Current position: guggulu may offer modest cholesterol benefit in standardised, high-quality preparations, but the evidence is less robust than for berberine or amla. It should be used under guidance — it interacts with several medications and can cause GI side effects. Triphala guggulu (combined with triphala) is the more commonly used Ayurvedic formulation, where triphala’s own lipid-modulating properties contribute to the combination’s effect.
⚗️ FXR antagonism → LDL receptor upregulation | Guggulsterone Z+E active compounds | Mixed clinical evidence — use standardised preparationsRegular aerobic exercise is the single most effective non-dietary intervention for improving the Indian atherogenic lipid profile — specifically because of its disproportionate benefit on the two parameters most abnormal in South Asians: low HDL and high triglycerides. Exercise raises HDL through multiple mechanisms: increasing the production of apolipoprotein A-I (the main structural protein of HDL), activating lecithin-cholesterol acyltransferase (which matures nascent HDL particles into mature, functional ones), and reducing the activity of hepatic lipase (which breaks down HDL). Regular aerobic exercise raises HDL by 5–10% — modest numerically, but significant given how low Indian adults’ baseline HDL typically is.
Triglycerides respond robustly to exercise: a single session of moderate-to-vigorous aerobic exercise reduces circulating triglycerides for 24–72 hours through enhanced lipoprotein lipase activity in muscle tissue. Consistent exercise (150+ minutes of moderate activity weekly) produces sustained triglyceride reduction of 10–20%. Resistance training adds further benefit through increased muscle mass — muscle is a primary site of triglyceride clearance through lipoprotein lipase.
A 2013 meta-analysis of 51 trials confirmed that regular aerobic exercise significantly reduced LDL by 5%, total cholesterol by 5%, triglycerides by 7%, and raised HDL by 3% — with all effects being dose-dependent (more exercise = more improvement). Walking 30 minutes daily is sufficient to produce measurable improvement within 3 months.
⚗️ HDL +3–10% | TG reduction 10–20% with consistent exercise | 51-trial meta-analysis 2013 | 24–72hr TG reduction after single sessionIn the context of the Indian diet — where refined carbohydrates (white rice, maida, packaged snacks, sugar, sweetened beverages) can constitute 60–70% of caloric intake — reducing refined carbohydrate intake is one of the most powerful interventions for the Indian atherogenic lipid profile. The mechanism: excess refined carbohydrates raise blood glucose and insulin, promoting hepatic de novo lipogenesis (the conversion of excess glucose to triglycerides and VLDL) and suppressing lipoprotein lipase activity (reducing triglyceride clearance). The resulting hyperinsulinaemia also reduces hepatic apolipoprotein A-I production, directly lowering HDL.
Practical implementation: replacing refined grain (white rice, maida roti) with whole grain, millets (ragi, bajra, jowar), and legumes reduces the glycaemic load of meals, blunts postprandial insulin, and produces sustained triglyceride reduction. Eliminating sweetened beverages (chai with 2 spoons of sugar × 4 cups = 40g sugar daily from chai alone) and packaged snacks provides the most immediate improvement. The PREDIMED study and multiple other large dietary trials confirm that replacing refined carbohydrates with healthy fats and protein improves the TG:HDL ratio — the most relevant cardiovascular risk marker for Indians.
Indian Foods for Cholesterol — Complete Quick Reference
| Indian Food | Primary Mechanism | Targets | Evidence Level | Best Form & Amount |
|---|---|---|---|---|
| Isabgol (psyllium husk) | Bile acid sequestration via viscous soluble fibre gel | LDL ↓ 5–7% | Very Strong (multiple meta-analyses) | 1 tbsp in water before main meal daily |
| Amla (Indian gooseberry) | HMG-CoA reductase inhibition + LDL oxidation prevention + insulin sensitisation | LDL ↓ 24%, TG ↓ 27%, HDL ↑ 14% | Strong (EJCN 2012 RCT) | 1–2 fresh daily or 1 tsp powder in warm water |
| Methi seeds (fenugreek) | Galactomannan bile acid binding + saponin cholesterol absorption inhibition | LDL ↓, TG ↓, HDL ↑ (modest) | Moderate–Strong (meta-analysis) | 1 tsp soaked overnight, eaten on empty stomach |
| Oats and barley | Beta-glucan soluble fibre — bile acid sequestration | LDL ↓ 5–10% | Very Strong (Cochrane reviewed) | Daily breakfast oatmeal or barley khichdi |
| Dal and legumes (all varieties) | Soluble fibre + plant protein + phytosterols — reduces LDL absorption + VLDL production | LDL ↓ 5–8%, TG ↓ | Very Strong (multiple trials) | 2 servings daily — main protein source |
| Walnuts (akhrot) | ALA omega-3 + gamma-tocopherol + phytosterols — VLDL reduction + LDL oxidation protection | LDL ↓ 5–9%, TG ↓ | Strong (multiple RCTs) | 5–7 walnuts daily |
| Flaxseed (alsi, ground) | ALA omega-3 + lignans (anti-atherogenic) + soluble fibre | LDL ↓ 4–8%, TG ↓ | Moderate–Strong (systematic review) | 1 tbsp ground in curd or roti daily |
| Til (sesame seeds) | Phytosterols + sesamin lignans (reduce cholesterol absorption + LDL oxidation) | LDL ↓, HDL ↑ (modest) | Moderate (clinical studies) | 1–2 tbsp daily — til chutney, ladoo, in cooking |
| Garlic (lahsun) | Allicin inhibits HMG-CoA reductase + reduces LDL oxidation + antithrombotic | LDL ↓ 9–12%, Total cholesterol ↓ | Moderate (meta-analysis, some inconsistency) | 2–4 raw cloves crushed daily (10 min activation before use) |
| Green tea | EGCG catechins reduce cholesterol absorption + LDL oxidation | LDL ↓ 5–6%, Total cholesterol ↓ | Moderate–Strong (meta-analysis) | 2–3 cups daily, 70–80°C, 3–5 min steep |
| Ragi, bajra, jowar (millets) | Low GI reduces postprandial insulin → less hepatic VLDL production; phytosterols | TG ↓, HDL ↑ (via TG:HDL improvement) | Moderate (GI + metabolic research) | Replace white rice/maida as staple grain |
| Turmeric + black pepper | Curcumin AMPK activation → reduces fatty liver + VLDL; anti-inflammatory on vascular endothelium | LDL ↓ (modest), TG ↓ (modest), HDL ↑ (modest) | Moderate (clinical studies) | ½ tsp in cooking with black pepper + fat always |
The Portfolio Diet — Combining Multiple Strategies for Maximum Effect
One of the most powerful concepts in natural cholesterol management is the “Portfolio Diet” — developed by Dr. David Jenkins at the University of Toronto — which demonstrates that combining multiple evidence-based dietary interventions produces additive effects significantly greater than any single intervention alone.
A landmark 2003 JAMA trial found that the Portfolio Diet — combining plant sterols (2g/day), soluble fibre (10g+/day), plant protein (soy, nuts), and nuts — reduced LDL by 28.6% in one month. This was statistically comparable to lovastatin (a standard statin medication) at 30.9% reduction. A 2011 multi-centre RCT confirmed that sustained Portfolio Diet adherence over 6 months reduced LDL by 13–17% in a community setting.
The Indian Portfolio Diet adaptation:
✓ Soluble fibre daily: oats at breakfast + dal at every meal + isabgol before dinner (10+ grams soluble fibre daily)
✓ Plant protein emphasis: dal, legumes, nuts, soy (tofu/edamame) as primary protein sources
✓ Plant sterols: til and pumpkin seeds daily, rice bran oil for cooking, targeted supplementation if needed
✓ Nuts: 5–7 walnuts + small handful of almonds daily
✓ Amla: daily (1–2 fresh or 1 tsp powder)
✓ Eliminate trans fats: remove vanaspati, dalda, commercial bakery products
✓ Replace refined grains: millets, whole wheat, barley for white rice and maida where possible
Combined estimated LDL reduction (Indian Portfolio): 20–30% within 3 months. This is clinically meaningful and may be sufficient for mild-moderate dyslipidaemia to avoid or defer statin therapy under medical supervision.
Cholesterol Myths vs. Facts — The Ones Causing Confusion in India
“High cholesterol only matters if you have symptoms.”
High cholesterol causes no symptoms — it is entirely silent until a heart attack or stroke occurs. This is why it is called a “silent killer.” Atherosclerosis builds over decades without causing pain or discomfort. The only way to know your cholesterol is with a blood test (fasting lipid profile). Every adult over 30 (or earlier with risk factors) should have a lipid profile done — not because they feel unwell, but precisely because they feel well.
“Eating egg yolks significantly raises cholesterol.”
Dietary cholesterol (the cholesterol you eat) has a much smaller effect on blood cholesterol than saturated and trans fat intake. The liver adjusts its own cholesterol production based on dietary intake — in most people, eating 1–2 eggs daily has minimal impact on LDL. For most healthy people, saturated fat from ghee, coconut oil, and full-fat dairy is far more important to manage than egg consumption. People with diabetes or existing cardiovascular disease should discuss egg intake with their physician — the relationship is more complex in these groups.
“If my total cholesterol is below 200, I don’t need to worry.”
Total cholesterol below 200 mg/dL is not a guarantee of low cardiovascular risk — particularly in Indians. The composition matters: total cholesterol of 180 with HDL of 30 and TG of 250 carries far higher cardiovascular risk than total cholesterol of 200 with HDL of 60 and TG of 90. Non-HDL cholesterol, TG:HDL ratio, Lp(a), and small dense LDL particle number are better risk predictors than total cholesterol alone for the Indian lipid profile.
“Statins are always unnecessary — natural remedies are sufficient.”
For people with existing cardiovascular disease, very high LDL (above 190 mg/dL), or very high cardiovascular risk, statins are among the most evidence-backed and life-saving medications available. The FOURIER and ODYSSEY trials show that for high-risk patients, aggressive LDL reduction prevents heart attacks and saves lives. Natural interventions are most appropriate for low-to-moderate risk individuals and as complementary therapy alongside statins. Rejecting statins based on side effect concerns that are often exaggerated in online content — without replacing them with equally effective alternatives — is a genuine health risk for high-risk individuals.
When Medical Evaluation and Treatment Are Essential
LDL is above 190 mg/dL: This level suggests possible familial hypercholesterolaemia (genetic high cholesterol) — a condition where lifestyle intervention alone rarely achieves target and statin therapy is typically indicated regardless of other risk factors.
LDL is above 100 mg/dL with existing cardiovascular disease (previous heart attack, stroke, or stent): Post-cardiovascular event, LDL target is <70 mg/dL — typically achievable only with medication in this context.
LDL is above 130 mg/dL with multiple risk factors (diabetes, hypertension, smoking, family history of premature heart disease, obesity): The 10-year cardiovascular risk calculation determines whether statin initiation is appropriate — discuss with your physician.
High Lp(a) with any cardiovascular risk: Lp(a) elevation is not addressable through lifestyle or standard medications. Emerging therapies (RNA interference agents) are in advanced clinical trials. Current management: aggressive reduction of all other modifiable risk factors as compensation.
Natural interventions are not a replacement for appropriate medical management in high-risk individuals. They are most powerful as first-line therapy for low-to-moderate risk and as complementary therapy that may allow lower medication doses for higher-risk individuals. Always discuss with your physician.
Frequently Asked Questions About Natural Ways to Lower Cholesterol
The fastest measurable LDL reductions come from: plant sterols 2g/day (10–15% LDL reduction in 2–3 weeks); eliminating trans fats (immediate benefit); isabgol husk daily (5–7% in 4–6 weeks); and berberine 500mg 2–3x daily (25% LDL reduction in 8–12 weeks). The Portfolio Diet approach combining soluble fibre, plant sterols, plant protein, and nuts produces 20–30% LDL reduction in one month — comparable to low-dose statin therapy. No single intervention achieves dramatic results in days; consistent application of combined strategies over 4–12 weeks produces clinically meaningful change.
The South Asian atherogenic lipid profile: lower HDL than Western populations even at similar total cholesterol, higher triglycerides, elevated Lp(a), and smaller denser LDL particles (more atherogenic per unit). This produces higher cardiovascular risk per unit of total cholesterol than in Western populations. Indian lipid targets should be calibrated lower. HDL-raising and TG-lowering strategies (exercise, omega-3, refined carbohydrate reduction) are as important as LDL lowering for the Indian cardiovascular risk profile.
Yes — a 2012 double-blind RCT in the European Journal of Clinical Nutrition found amla (500mg twice daily) reduced LDL by 24%, triglycerides by 27%, and increased HDL by 14%. The mechanism: HMG-CoA reductase inhibition (statin-like), Vitamin C prevents LDL oxidation, and chromium improves insulin sensitivity (reducing VLDL). Daily amla (fresh, powder, or standardised extract) is one of the most evidence-backed natural cholesterol interventions available for Indians.
Best Indian foods for cholesterol: isabgol (5–7% LDL), amla (24% LDL, 27% TG, 14% HDL increase per 2012 RCT), methi seeds (TG + LDL reduction), oats and barley (beta-glucan, 5–10% LDL), all dal and legumes (daily staple with cholesterol benefit), walnuts 5–7 daily, ground flaxseed 1 tbsp, til/sesame seeds, garlic (2–4 raw crushed cloves daily), green tea 2–3 cups, and millets (ragi/bajra/jowar) to replace refined grains and reduce TG:HDL ratio.
For mild-to-moderate cholesterol elevation without existing cardiovascular disease, the Portfolio Diet approach can reduce LDL by 20–30% — comparable to low-dose statin therapy. For people with very high LDL, existing cardiovascular disease, or very high overall risk, statins are essential and should not be deferred. Natural interventions are best as first-line for low-to-moderate risk and as complementary therapy for higher-risk individuals already on medication. Always discuss with your physician — the combination of lifestyle change and medication produces better outcomes than either alone.
LDL (“bad” cholesterol — target <100 mg/dL): deposits cholesterol in arterial walls, driving atherosclerosis. HDL (“good” cholesterol — target >50 mg/dL women, >40 mg/dL men): removes cholesterol from arteries back to the liver. Triglycerides (target <150 mg/dL): blood fats elevated by refined carbohydrates, alcohol, and insulin resistance — independently increase cardiovascular risk, particularly in Indians. Non-HDL cholesterol (total minus HDL — target <130 mg/dL) is a more comprehensive risk marker for Indians, capturing VLDL and IDL as well as LDL. The TG:HDL ratio is one of the most sensitive insulin resistance and cardiovascular risk markers for South Asians.
Related Articles You’ll Love
The Indian lipid profile is not a Western problem with Indian packaging. It is a distinct metabolic pattern — low HDL, high triglycerides, elevated Lp(a), small dense LDL — that requires India-specific thinking. The interventions that matter most are not necessarily the ones that get the most attention: soluble fibre, plant sterols, amla, berberine, exercise for HDL and TG, and the replacement of refined grains with millets address the exact profile that drives India’s cardiovascular epidemic.
The Indian kitchen had the ingredients for decades — isabgol, methi, amla, til, dal, ragi. The science has now provided the mechanisms. The combination of both is one of the most powerful natural cardiovascular protection strategies available.
Start with your lipid panel. Know your numbers. Build your strategy from your kitchen outward. 🌿Which natural cholesterol strategy surprised you most — the amla RCT data (LDL -24%, HDL +14%), the Portfolio Diet’s statin-equivalent LDL reduction, or the berberine PCSK9-independent LDL receptor mechanism? Share this with every family managing cholesterol with diet — the evidence-backed approach makes all the difference. 👇
Sources & Further Reading
- Annals of Internal Medicine (2014) — Meta-analysis: Soluble Fibre and LDL Cholesterol Reduction (67 RCTs)
- JAMA (2003) — Jenkins et al.: Portfolio Diet vs Statin — Equivalent LDL Reduction
- European Journal of Clinical Nutrition (2012) — Amla RCT: Comprehensive Lipid Improvement (LDL -24%, TG -27%, HDL +14%)
- Nature Medicine (2004) — Berberine: LDL Receptor Upregulation, 25% LDL Reduction
- Plant Sterols Meta-analysis — 41 RCTs: 10–15% LDL Reduction at 2g/day
- Cochrane Review (2015) — Saturated Fat Reduction and Cardiovascular Events: 17% Risk Reduction
- Journal of Applied Physiology (2013) — Exercise and Lipids: 51-Trial Meta-analysis
- HerbeeLife — Heart Attack Warning Signs: Lp(a) and South Asian Cardiovascular Risk
- HerbeeLife — Natural Health & Ayurvedic Wellness
Disclaimer: This content is for informational purposes only and does not constitute medical advice. High cholesterol and cardiovascular risk require professional medical assessment and individualised management. Never discontinue prescribed cholesterol medication without physician guidance. Always consult your healthcare provider before starting new supplements, especially if on existing medications. Read full disclaimer →

