We go significantly beyond the standard “laser is minimally invasive and has a quick recovery” framing into the actual mechanisms — the internal sphincter spasm physiology of chronic fissures, the abscess-to-fistula progression, why fistulas cannot heal without intervention, and what specifically laser energy does to the fistula tract in the FiLaC procedure. Understanding your condition is the foundation of choosing the right treatment.
Anal Fissure vs. Anal Fistula — Two Distinct Conditions, Often Confused
Fissures and fistulas are both anorectal conditions that cause pain, bleeding, and discharge — but they are anatomically distinct, caused by different mechanisms, and require different treatments. Understanding the difference is the first step to appropriate management.
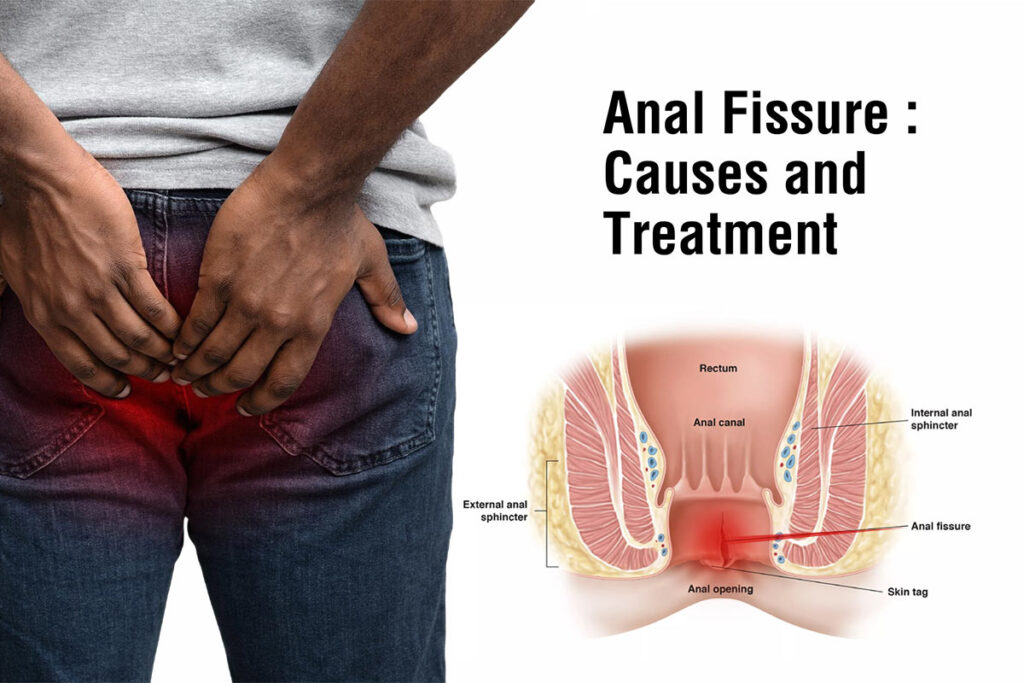
Anal Fissure: A small tear or crack in the lining (anoderm/mucosa) of the anal canal — typically at the posterior midline (6 o’clock position), less commonly at the anterior midline (12 o’clock). The tear occurs when the passage of a hard, large, or forceful stool stretches the anal canal beyond its elastic limit. The hallmark symptom: intense, sharp pain during and immediately after bowel movements (described by patients as “passing broken glass” or “sitting on fire”), followed by a dull throbbing ache that can last 1–4 hours. Bright red rectal bleeding — on the toilet paper or dripping after the stool — is common. The pain makes subsequent bowel movements feared, leading to further stool hardening and a vicious cycle of constipation worsening the fissure.
Anal Fistula: An abnormal tract (tunnel) connecting the inside of the anal canal (typically at the level of the dentate line, where anal glands open) to the skin surface around the anus. Almost always develops when a perianal abscess — an infected anal gland — does not fully resolve. The abscess drains spontaneously or surgically, but the infected gland creates a persistent tract lined with epithelium (skin cells) that the body cannot eliminate naturally. Symptoms: chronic intermittent discharge of pus or blood-stained fluid from a small opening on the perineal skin, recurrent perianal pain and swelling, wet skin causing irritation and itching, and relief of acute pain when the abscess spontaneously drains.
The critical difference for treatment decisions: Acute anal fissures often heal with conservative management. Anal fistulas virtually never heal without intervention — the epithelialised tract maintains itself and will continue to discharge and recur unless it is eliminated. Attempting to manage an established fistula with antibiotics alone, without addressing the underlying tract, produces temporary improvement followed by inevitable recurrence.
Anal Fissures — The Biology, Stages, and Why Chronic Fissures Don’t Heal Alone
An acute fissure (less than 6 weeks duration) can heal with conservative management because the tissue injury is fresh and the blood supply is adequate for repair. A chronic fissure develops when the initial tear triggers a vicious cycle that prevents healing: the pain of the fissure causes reflexive internal anal sphincter (IAS) spasm — the sphincter tightens in response to the painful stimulation. This IAS hypertonia (abnormally elevated resting sphincter pressure) significantly reduces blood flow to the posterior midline of the anal canal (the watershed area with the poorest blood supply even under normal conditions). Reduced blood flow means reduced oxygen and nutrient delivery to the healing wound — and the fissure cannot repair itself despite the body’s attempts.
Over weeks, the edges of the chronic fissure develop fibrotic (scar-like) changes; a swollen skin tag (sentinel pile) develops at the outer edge; and a hypertrophied anal papilla develops at the inner edge. These are the pathognomonic signs of a chronic fissure — and they indicate that conservative management alone has low probability of success. The fibrotic edges cannot heal without being refreshed, and the IAS hypertonia must be addressed.
This physiology explains every treatment modality: Topical nitrates and calcium channel blockers work by chemically relaxing IAS spasm. Botulinum toxin injection paralyses the IAS, giving it 3–4 months to heal. Lateral internal sphincterotomy (LIS) surgically cuts part of the IAS. Laser treatment addresses the fibrotic tissue at the base of the fissure. All are targeting the same physiological problem — IAS hypertonia as the barrier to healing.
⚗️ IAS hypertonia → reduced posterior midline blood flow → healing failure | Sentinel pile + hypertrophied papilla: chronic fissure signsAnal fissures are most common in young to middle-aged adults — they are the most common cause of rectal bleeding in infants and young children, and extremely common after childbirth (particularly following instrumental deliveries or large babies). In adults, the primary risk factors are chronic constipation (low dietary fibre, inadequate hydration, sedentary lifestyle), frequent diarrhea (paradoxically — repeated passage of loose stool irritates the anoderm), and the sitting toilet position that increases defecatory straining.
Fissures not at the posterior or anterior midline (called atypical or lateral fissures) should raise suspicion for underlying conditions: Crohn’s disease, ulcerative colitis, HIV/AIDS, tuberculosis, sexually transmitted infections, or anal malignancy. Any fissure that does not respond to standard treatment, is in an unusual location, or is associated with other symptoms (weight loss, night sweats, diarrhoea) requires further investigation rather than continued empirical treatment.
⚗️ Posterior midline 85–90% | Anterior midline common in women post-delivery | Lateral/atypical fissures → investigate for Crohn’s, TB, malignancyAnal Fistulas — The Abscess-to-Fistula Pathway and Sphincter Anatomy That Drives Treatment Choice
Approximately 90% of anal fistulas originate from infected anal glands — small glands located at the dentate line (the junction between the internal and external anal canal) that normally secrete lubricating fluid. When one of these glands becomes obstructed by faecal material and secondarily infected, it produces a perianal abscess — typically presenting as a painful, rapidly expanding swelling near the anus, with fever and significant pain. The abscess may drain spontaneously or require surgical incision and drainage.
In approximately 50% of cases, the drained or spontaneously opened abscess leaves behind a persistent fistula tract — the infected gland at the dentate line continues to act as the internal opening (primary source of infection), and the abscess drainage site becomes the external opening. The tract between these two points becomes lined with granulation tissue and eventually epithelium, producing a self-maintaining tunnel that continuously reinfects itself through the internal opening and drains through the external opening.
The Parks Classification categorises fistulas by their relationship to the sphincter complex: intersphincteric (most common — 70%, passes between the internal and external sphincters), transsphincteric (passes through both sphincters — treatment more complex), suprasphincteric, and extrasphincteric. This classification determines which treatment approaches are safe — the critical concern being preservation of sphincter function (continence).
⚗️ Cryptoglandular origin: 90% | 50% perianal abscess → fistula | Parks Classification: sphincter involvement determines treatmentTreatment Options — Natural, Ayurvedic, Laser, and Surgical: When to Choose Each
The treatment decision for anal fissures and fistulas is not one-size-fits-all. Condition type, duration, severity, sphincter anatomy, and patient preference all determine the optimal approach. The following covers the full spectrum from conservative to surgical.
For acute anal fissures (less than 6 weeks duration), conservative management achieves healing in the majority of patients — with studies suggesting 45–60% complete healing at 6–8 weeks with lifestyle modification alone, rising to 70–80% when topical medications are added. The natural management principles:
Dietary fibre: The single most important intervention — increasing dietary fibre to 25–35g daily softens stool and reduces anal canal pressure during defecation, directly addressing the mechanical cause of the fissure. Indian sources: ragi, whole wheat roti, isabgol husk, raw vegetables, seasonal fruits, and all varieties of dal and legumes. A 2011 Cochrane review confirmed that fibre supplementation significantly improves fissure healing and reduces recurrence. Read more about natural digestion improvement: Boost Digestion Naturally
Hydration: 2–2.5 litres of water daily — dehydration is among the most common causes of the hard stool that initiates and perpetuates fissures. In Indian summer months, increased fluid intake is particularly critical.
Warm sitz baths: Sitting in warm water (40–42°C) for 10–15 minutes after each bowel movement reduces IAS spasm (warmth relaxes smooth muscle), improves blood flow to the anal canal, and provides meaningful pain relief. Multiple randomised studies confirm sitz baths reduce pain scores and improve patient comfort significantly.
Defecatory position: Using a footstool (25–30cm) to raise the feet while on the toilet changes the anorectal angle toward the squatting position — reducing straining and anal canal pressure during defecation. The physiological basis: the puborectalis muscle (which maintains the anorectal angle and remains contracted during sitting) relaxes more completely in the squatting position, straightening the rectum and facilitating easier passage. This single change measurably reduces time spent on the toilet and straining effort.
Topical anaesthetic gel: Lidocaine 2.5% gel applied before bowel movements reduces the anticipated pain and the IAS spasm reflex triggered by the pain — breaking one link in the chronic fissure cycle. Available over the counter in India.
When conservative management alone does not achieve healing after 4–6 weeks, topical medications that specifically target IAS hypertonia are the established next step — prior to considering any procedural intervention.
Topical nitroglycerin (GTN) 0.2–0.4%: Works by releasing nitric oxide, which relaxes IAS smooth muscle — reducing IAS pressure by 30–40% and improving blood flow to the ischiorectal area. Multiple meta-analyses confirm significantly higher healing rates than placebo. Primary limitation: headache in 20–40% of patients (dose-related). Applied 2–3 times daily for 6–8 weeks. Healing rates: 50–75% in randomised trials. Available in India as prescription-only.
Topical diltiazem 2% (calcium channel blocker): Alternative to GTN with equivalent healing rates and significantly fewer headaches. Applied twice daily. Better tolerated, making it the preferred topical agent in most current guidelines. Healing rates: 65–75%. Available in India as a compounded preparation from certain pharmacies.
Botulinum toxin (Botox) injection: Injection directly into the IAS produces temporary chemical sphincterotomy — paralysing the overactive sphincter for 3–4 months, allowing the fissure to heal in the absence of hypertonicity. Success rates: 70–80% for chronic fissures that did not respond to topical treatment. Temporary — if the fissure recurs after Botox effect wears off, a second injection or surgical intervention may be needed. No risk of permanent incontinence.
⚗️ GTN: 30–40% IAS pressure reduction, 50–75% healing | Diltiazem: equivalent healing, fewer headaches | Botox: 70–80% success, temporary chemical sphincterotomyFor anal fissures: Laser treatment (typically diode laser, 980nm wavelength) for chronic fissures uses laser energy to achieve several simultaneous therapeutic effects: vaporisation of the fibrotic scar tissue at the base of the fissure (refreshing the wound edges for better healing potential), thermal relaxation of the superficial IAS fibres (addressing hypertonia without the precision and deliberateness of surgical sphincterotomy), removal of the sentinel skin tag and hypertrophied anal papilla (the anatomical markers of chronicity), and stimulation of collagen remodelling through controlled thermal injury to the healing bed.
The procedure is performed under local anaesthesia (perianal block) with or without mild sedation, takes approximately 20–30 minutes, and is typically day-case. Multiple Indian and international series report healing rates of 80–90% for chronic fissures treated with laser — comparable to or slightly superior to LIS in several published studies, with a significantly lower risk of faecal incontinence (the primary serious complication of LIS).
For anal fistulas — the FiLaC procedure (Fistula Laser Closure): A thin, flexible laser probe (radially emitting diode laser fibre) is inserted through the external opening and advanced along the fistula tract. As the probe is withdrawn slowly, the laser energy (delivered circumferentially at 360°) destroys the epithelialised lining of the fistula tract, causes thermal contraction and obliteration of the tract, and promotes healing by secondary intention. The internal opening is simultaneously closed with a small mucosal advancement flap or suture. The sphincter complex is NOT cut — making FiLaC sphincter-preserving and essentially eliminating the incontinence risk associated with conventional fistulotomy.
FiLaC outcomes — the honest picture: Primary healing rates for FiLaC across published series: 60–80% for simple intersphincteric fistulas, 50–70% for transsphincteric fistulas. These are lower than open fistulotomy (which has 90%+ healing for simple fistulas) but with dramatically lower incontinence risk. FiLaC is most appropriate for: complex or high fistulas where conventional surgery carries significant incontinence risk, patients who are highly concerned about incontinence risk, and as a repeatable procedure (can be performed multiple times without progressive sphincter damage). For simple low intersphincteric fistulas in young patients, conventional fistulotomy may offer better single-treatment cure rates.
⚗️ Fissure laser: 80–90% healing, lower incontinence risk than LIS | FiLaC: 60–80% simple, 50–70% complex fistulas | Sphincter-preserving mechanismKshar Sutra is the single most important uniquely Indian contribution to the treatment of anal fistula — and one of the most clinically important Ayurvedic procedures with rigorous modern validation. The procedure involves passing a linen thread coated with a standardised alkaline paste (made from the ash of Apamarga — Achyranthes aspera — combined with latex of Snuhi — Euphorbia neriifolia — and turmeric) through the entire fistula tract from internal to external opening, then tying the ends together as a loop around the sphincter-containing tissue.
The thread is changed weekly in the clinic. Over 5–10 weeks (depending on the depth of the fistula), the alkaline paste slowly cuts through the fistula tissue at a rate of approximately 0.5–1cm per week, while simultaneously stimulating healing and fibrosis behind the cutting front. Because the cutting is gradual, the sphincter tissue ahead of the thread has time to form fibrosis and mature — preventing the sudden dehiscence that causes incontinence in rapid conventional cutting procedures.
The ICMR validation: A landmark 1991 randomised controlled trial conducted by the Indian Council of Medical Research (ICMR) specifically compared Kshar Sutra to conventional fistulotomy for anal fistula. The results: Kshar Sutra achieved a recurrence rate of 3.33% versus 11.33% for conventional surgery — statistically significant superiority. The WHO subsequently recognised Kshar Sutra as a valid treatment for anal fistula. Multiple subsequent clinical studies have confirmed lower recurrence rates and comparable or superior continence preservation compared to conventional surgery.
Advantages: Can be performed as an outpatient procedure under local anaesthesia. No hospitalisation required. Gradual cutting preserves continence for high/complex fistulas. Very low recurrence rate. Cost-effective. Widely available in India at Ayurvedic hospitals and proctology centres. Disadvantages: Longer treatment duration (6–12 weeks of weekly visits) compared to single-session laser or surgical procedures. Some discomfort during and after thread changes. Not appropriate for complex multi-tract fistulas without modification.
Lateral Internal Sphincterotomy (LIS) for chronic anal fissures: Surgical division of a portion of the internal anal sphincter at the 3 or 9 o’clock position (lateral, not at the site of the fissure — avoiding the posterior midline scar). LIS remains the most effective treatment for chronic anal fissure, with healing rates of 95%+ in most series. It addresses the root cause directly — the IAS hypertonia — by permanently reducing IAS pressure. The primary concern: risk of minor faecal incontinence (gas or liquid stool incontinence) in approximately 5–10% of patients in long-term follow-up, higher in women with prior obstetric sphincter injury. This risk has driven the development of Botox injection and laser alternatives for patients who prioritise continence preservation.
Fistulotomy for anal fistulas: Laying open the entire fistula tract (cutting through the tissue overlying it) allows the wound to heal from the bottom up. For simple, low-lying intersphincteric fistulas that do not involve significant sphincter, fistulotomy has healing rates exceeding 90% with a single procedure and is the gold standard. For fistulas involving the external sphincter or higher (transsphincteric, suprasphincteric), fistulotomy carries significant incontinence risk — which is why sphincter-preserving alternatives (Kshar Sutra, FiLaC, LIFT procedure, advancement flap) are preferred for these complex cases.
⚗️ LIS: 95%+ healing, 5–10% minor incontinence risk | Fistulotomy: 90%+ for simple fistulas | Complex fistulas: sphincter-preserving approach requiredTreatment Comparison — Fissures and Fistulas at a Glance
| Treatment | Best For | Healing Rate | Incontinence Risk | Recovery Time | Procedure Time |
|---|---|---|---|---|---|
| Conservative (fibre + sitz bath + GTN/diltiazem) | Acute fissures (<6 weeks) | 70–80% with topical medication | None | 6–8 weeks for healing | N/A — home treatment |
| Botulinum toxin injection | Chronic fissure, moderate case | 70–80% | Minimal (temporary) | 2–4 weeks | 15 minutes, outpatient |
| Laser (fissure) | Chronic fissure, failed conservative | 80–90% | Very low | 1–2 weeks | 20–30 min, day-case |
| LIS (Lateral Internal Sphincterotomy) | Chronic fissure, failed all else | 95%+ | 5–10% minor risk | 2–3 weeks | 30–45 min, day-case |
| Kshar Sutra | All fistulas, especially complex | Low recurrence (3–5%) | Very low (gradual cutting) | 6–12 weeks (outpatient visits) | 30–45 min + weekly changes |
| FiLaC (laser fistula closure) | Complex/high fistulas, recurrent | 60–80% (simple), 50–70% (complex) | Minimal (sphincter-preserving) | 2–3 weeks | 45–60 min, day-case |
| Fistulotomy (conventional) | Simple, low intersphincteric fistulas | 90%+ | Low for simple, higher for complex | 4–8 weeks wound healing | 30–60 min, usually day-case |
Indian Home Remedies for Anal Fissures — What Works and Why
Isabgol (psyllium husk, Plantago ovata) is the most evidence-backed natural stool softener for fissure management. Its soluble fibre absorbs water in the colon, forming a viscous gel that softens and bulks stool, reducing the anal canal pressure during defecation that caused and perpetuates the fissure. A 2006 meta-analysis confirmed that soluble fibre supplementation reduces constipation severity, straining, and — in a study specifically including fissure patients — improves healing rates and reduces recurrence.
Mix 1–2 tsp isabgol in a large glass of water and drink immediately before it gels (it becomes very thick very quickly). Always take with at least 250ml of additional water — insufficient fluid makes isabgol counter-productive. Best taken at bedtime so stool softens overnight for an easier morning bowel movement. Continue throughout fissure treatment and beyond — relapse is common when isabgol is stopped and dietary fibre reverts to prior inadequate levels.
⚗️ Soluble fibre gel → stool softening and bulking | Reduces anal canal pressure during defecation | Take with adequate fluid alwaysWarm sitz baths — sitting in warm water (40–42°C) in a tub, bucket, or specialised sitz bath basin for 10–15 minutes after each bowel movement — are the most evidence-backed non-pharmacological pain management strategy for anal fissures. The mechanism: warm water relaxes the internal anal sphincter smooth muscle (reducing IAS spasm and pain), improves blood circulation to the anorectal area (promoting tissue oxygenation and healing), cleanses the anal area gently (reducing secondary infection), and provides direct comfort through thermoreceptor activation. Adding 1–2 tablespoons of Epsom salt (magnesium sulphate) to the sitz bath water provides additional muscle relaxation through transdermal magnesium absorption and creates a mildly antiseptic solution. In India, adding 2–3 neem leaves to the water provides gentle antimicrobial benefit aligned with traditional practice.
⚗️ Warm water → IAS smooth muscle relaxation | Improved blood flow to healing tissue | 3x daily during acute fissure phaseTwo readily available Indian kitchen and home ingredients have documented topical benefit for anal fissures. Coconut oil: its primary fatty acid (lauric acid, 50% of coconut oil) has documented anti-inflammatory and antimicrobial properties. Applied topically to the anal area after sitz baths, coconut oil lubricates the anal canal (reducing mechanical trauma during defecation), provides anti-inflammatory benefit through lauric acid, and forms a protective barrier. A 2018 clinical review noted coconut oil’s wound-healing properties, including improved collagen synthesis and anti-inflammatory effects on dermal wounds. Aloe vera gel: the inner leaf gel of Aloe barbadensis contains polysaccharides (acemannan) that promote fibroblast activity and collagen synthesis, and anthraquinones with anti-inflammatory and mild antimicrobial activity. Applied gently to the anal area, aloe vera gel soothes the irritated mucosa and supports healing. Use fresh gel from the plant (scoop from a broken aloe leaf) or pure, unfragranced commercial aloe gel.
Anal fissures in most Indian patients are ultimately caused by the same thing: hard stool from insufficient dietary fibre and inadequate hydration, sometimes combined with a sedentary lifestyle reducing colonic motility. No topical cream, no Botox, no laser, and no surgery will provide lasting benefit if the root causes are not addressed — because the fissure will heal and then recur with the next episode of constipation.
The fibre imperative: Most Indian adults consume 10–15g of dietary fibre daily — half to two-thirds of the 25–35g recommended. Practical increases: switch from refined wheat roti to whole wheat or multigrain; eat at least 2 servings of vegetables per meal; include whole dal (with husk) rather than split dal; add a piece of fresh fruit daily; and take isabgol husk as a supplement until dietary fibre is adequate. Ragi (finger millet) at 3.6g fibre/100g is among the best Indian grain sources for those wanting to increase fibre through regular food rather than supplements.
The hydration imperative: 2–2.5 litres of fluid daily. The first glass of water should be drunk immediately on waking — cold water stimulates the gastrocolic reflex (the colonic motor response to stomach distension) and promotes a morning bowel movement at a physiologically optimal time.
The defecatory habit: Never postpone the urge to defecate — suppression hardens stool and makes defecation more traumatic. Spend maximum 3–5 minutes on the toilet — prolonged sitting increases anorectal pressure and promotes engorgement of haemorrhoidal tissue. Use a footstool to achieve a semi-squatting position. Do not use mobile phones or read on the toilet — this extends sitting time significantly.
⚗️ Root cause: low fibre + low hydration | Gastrocolic reflex: morning water for optimal defecation timing | Max 3–5 min toilet timeMyths vs. Facts — Common Misconceptions About Fissures and Fistulas
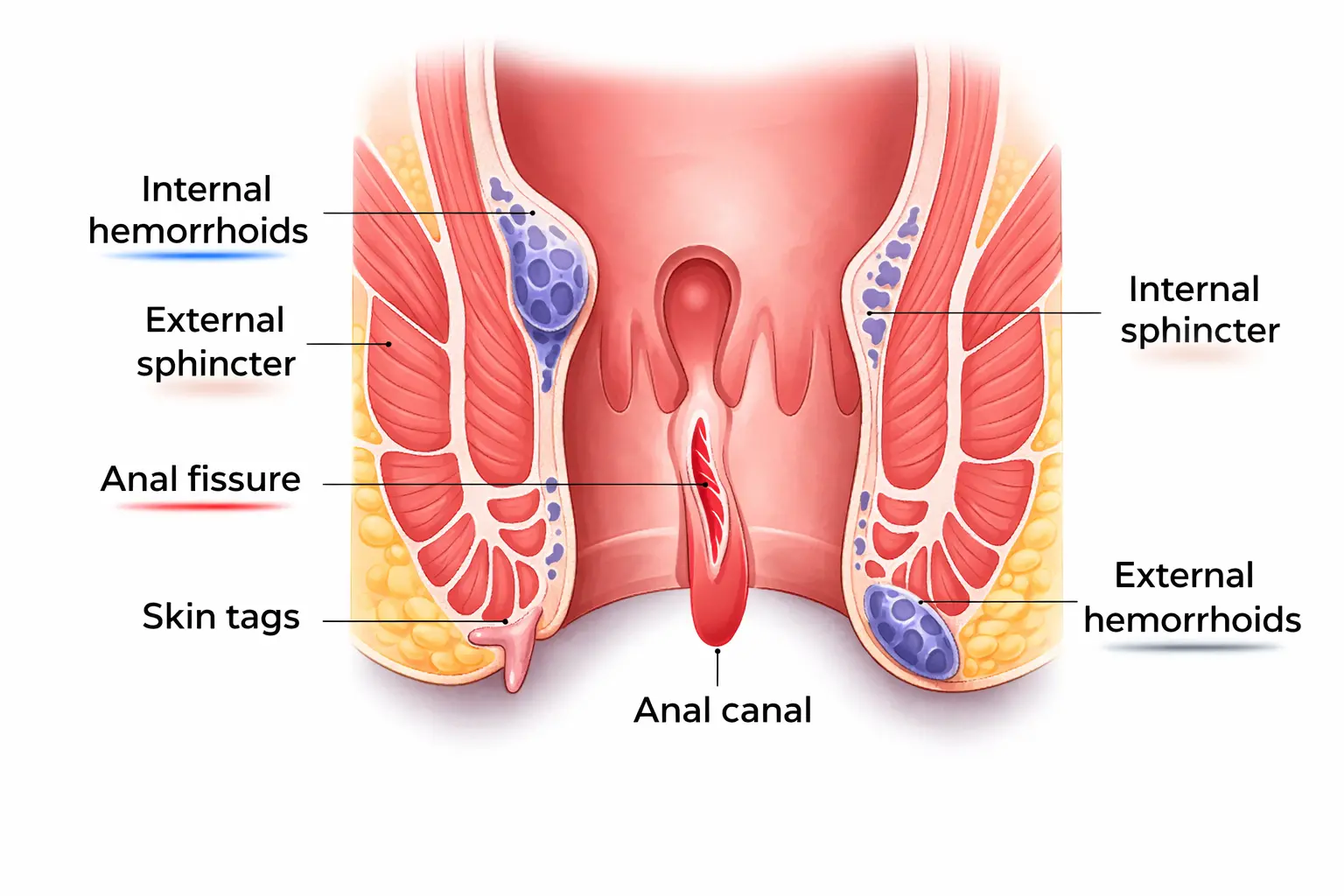
“Anal fissure and piles (haemorrhoids) are the same condition.”
These are entirely different conditions. Haemorrhoids are swollen blood vessels in the anal canal and perianal area — they cause bright red bleeding and prolapse but typically mild discomfort. Anal fissures are tears in the anal canal lining — they cause severe pain during and after bowel movements. Both can cause rectal bleeding. Both can coexist. But they have different mechanisms, different treatments, and different outcomes. Do not assume bright red rectal bleeding is necessarily haemorrhoids without evaluation — both fissures and, importantly, colorectal cancer require consideration.
“An anal fistula can heal on its own with antibiotics and wound dressings.”
Established anal fistulas with a defined tract virtually never heal spontaneously or with antibiotics. The tract becomes epithelialised (lined with skin cells that maintain it permanently), and the internal opening continues to allow gut contents into the tract. Antibiotics suppress the acute infection but do not eliminate the tract — the fistula recurs when antibiotics are stopped. Definitive treatment (Kshar Sutra, FiLaC, or conventional surgery) is required to permanently eliminate the tract.
“Surgery for fissures and fistulas always causes incontinence.”
Significant faecal incontinence from modern fissure and fistula surgery is uncommon when procedures are performed by experienced colorectal surgeons with appropriate technique. LIS for fissures carries approximately 5–10% minor incontinence risk (mainly flatus or occasional liquid stool) — severe incontinence is rare. For simple fistulas, fistulotomy carries very low incontinence risk. For complex fistulas, sphincter-preserving approaches (Kshar Sutra, FiLaC, LIFT) specifically avoid this risk. An experienced surgeon assessing the anatomy before surgery significantly reduces this concern.
“Any bright red rectal bleeding is just piles — no need to see a doctor.”
Bright red rectal bleeding requires medical evaluation — particularly in people over 40, anyone with a change in bowel habits, anyone with bleeding persisting beyond 2 weeks, or anyone with associated symptoms (weight loss, anaemia, abdominal pain). While haemorrhoids are the most common cause of bright red rectal bleeding, colorectal cancer — the third most common cancer in Indian men — can present with rectal bleeding and is frequently attributed to haemorrhoids without appropriate investigation, delaying diagnosis.
When to See a Doctor — Warning Signs That Require Prompt Evaluation
Any rectal bleeding in a person over 40 — even if it seems obviously related to haemorrhoids or fissures. Colorectal cancer must be excluded, particularly with any associated change in bowel habit, weight loss, or anaemia.
Fissure symptoms not improving after 4–6 weeks of consistent conservative management (fibre, hydration, sitz baths, topical medication). Chronic fissures require physician assessment for topical prescriptions and possible procedural intervention.
A painful perianal swelling that is hot and tender — this may be a perianal abscess requiring incision and drainage. Untreated perianal abscesses spread rapidly and can cause necrotising fasciitis (life-threatening). Do not attempt to manage perianal abscesses at home.
Perianal discharge of pus or blood-stained fluid from a small opening near the anus — this is an anal fistula that requires formal assessment and planning for definitive treatment.
Fissure symptoms in unusual locations (not posterior or anterior midline), or fissures not healing after full appropriate treatment, warrant investigation for Crohn’s disease, tuberculosis, HIV, or other systemic causes.
All anorectal conditions are treatable. Delay causes progression to more complex disease requiring more extensive intervention. Early assessment — despite the discomfort of the consultation — produces far better outcomes.
Frequently Asked Questions About Anal Fissures and Laser Surgery for Fistulas
An anal fissure is a tear in the anal canal lining — causing sharp pain during bowel movements and bright red bleeding. Most acute fissures (under 6 weeks) can heal with conservative management. An anal fistula is an abnormal tract connecting the inside of the anal canal to the skin around the anus — caused by an unresolved perianal abscess. It causes chronic discharge of pus or blood, recurrent swelling, and itching. Fistulas do not heal without definitive intervention (Kshar Sutra, FiLaC, or conventional surgery). These are distinct conditions requiring different treatment approaches.
Yes — most acute fissures (under 6 weeks) heal with conservative management: high dietary fibre (25–35g daily), adequate hydration (2+ litres daily), warm sitz baths after bowel movements, topical anaesthetic gel, and topical nitrate or calcium channel blocker cream (prescribed). Healing rates: 70–80% with full conservative management. Chronic fissures (over 6–8 weeks, with sentinel pile and fibrotic edges) have lower conservative healing rates — Botox injection, laser treatment, or lateral internal sphincterotomy may be needed. Natural management with isabgol, sitz baths, triphala, aloe vera, and coconut oil addresses both the fissure and the underlying constipation that caused it.
Laser treatment uses concentrated laser energy (typically diode 980nm) to vaporise the fibrotic scar tissue at the chronic fissure base, release IAS spasm thermally, remove the sentinel skin tag and hypertrophied papilla, and stimulate collagen remodelling. Performed under local anaesthesia, 20–30 minutes, day-case. Healing rates 80–90% for chronic fissures — comparable to LIS (lateral internal sphincterotomy) with lower incontinence risk. The advantage over LIS: precision, minimal tissue damage, and significantly lower risk of the 5–10% minor incontinence associated with LIS.
Kshar Sutra is an Ayurvedic procedure where a medicated thread (coated with Apamarga alkaline paste, Snuhi latex, and turmeric) is passed through the fistula tract and changed weekly. The alkaline paste slowly cuts through the tract over 6–12 weeks while simultaneously promoting healing — allowing sphincter tissue to fibrosis synchronously, preserving continence. A 1991 ICMR randomised trial found Kshar Sutra superior to conventional surgery for fistula — 3.33% recurrence vs 11.33%. WHO-recognised. Particularly valuable for complex fistulas where conventional surgery carries high incontinence risk. Widely available at Ayurvedic and proctology hospitals across India.
Laser fissure treatment: mild discomfort 3–7 days, desk work return in 2–3 days, full activity in 1–2 weeks. FiLaC (laser fistula closure): mild wound drainage 2–4 weeks during tract healing, return to light work in 3–5 days, full activity in 2–3 weeks. Both: maintain high-fibre diet and 2+ litres hydration during recovery. Warm sitz baths after each bowel movement for 2–4 weeks. Local anaesthetic gel before bowel movements helps during recovery. Complete the full recovery protocol — early return to hard physical work or straining can compromise results.
The most evidence-backed Indian home remedies for fissures: isabgol husk (psyllium — most effective stool softener, 1–2 tsp in water at bedtime), warm sitz baths 10–15 minutes after each bowel movement (IAS spasm relief + blood flow improvement), triphala churna in warm water at bedtime (gentle laxative + anti-inflammatory), aloe vera gel applied topically (anti-inflammatory, wound healing), coconut oil applied topically (anti-inflammatory, lubricating, protective), and ragi/whole grain dal as dietary base (high fibre from food). These address both the fissure itself and the underlying constipation that caused it. Continue all lifestyle interventions after healing to prevent recurrence.
Related Articles You’ll Love
Anal fissures and fistulas are among the most treatable conditions in medicine — yet among the most commonly delayed in treatment, because stigma and discomfort prevent people from seeking the evaluation they need. The natural remedies that prevent and support healing are already in your kitchen — isabgol, triphala, aloe vera, warm water, and whole grains. The traditional Ayurvedic intervention (Kshar Sutra) has ICMR-validated superiority over conventional surgery for fistulas and is available across India. The laser procedures offer precision, speed, and sphincter preservation unavailable a decade ago. And simple lifestyle changes — more fibre, more water, fewer minutes on the toilet — prevent the constipation that causes most fissures in the first place.
These conditions do not resolve by being ignored. But they respond beautifully to the right intervention — natural, Ayurvedic, or surgical — when sought at the right time.
Start with your kitchen. See a doctor when needed. Choose treatment with confidence. 🌿Which part of this guide was most useful — the fissure vs. fistula distinction, the Kshar Sutra ICMR data, or the natural home remedies with mechanisms? Share this with anyone who has been silently managing these conditions without knowing all their options. 👇
Sources & Further Reading
- Cochrane Review (2011) — Bulking Agents, Antispasmodics and Antidepressants for the Treatment of Irritable Bowel Syndrome and Fibre for Constipation
- Colorectal Disease (2012) — FiLaC (Fistula Laser Closure): Technique and Outcomes
- Indian Council of Medical Research (ICMR 1991) — Kshar Sutra vs. Conventional Surgery for Anal Fistula: Randomised Controlled Trial
- Techniques in Coloproctology (2009) — Laser Sphincterotomy for Chronic Anal Fissure: Prospective Study
- Diseases of the Colon and Rectum (2004) — Parks Classification of Anal Fistulas and Treatment Algorithm
- ASCRS Practice Parameters — Diagnosis and Management of Anal Fistulas (2016)
- HerbeeLife — Boost Digestion Naturally: 10 Science-Backed Home Remedies
- HerbeeLife — Natural Health & Ayurvedic Wellness
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Anal fissures and fistulas require professional diagnosis and individualised treatment planning. Please consult a qualified colorectal surgeon, gastroenterologist, or Ayurvedic specialist for personalised assessment and treatment recommendations. Read full disclaimer →

