We go past the standard “eat more tomatoes and exercise” advice into the actual biology of BPH — the DHT pathway that drives prostatic growth, the inflammatory component that determines symptom severity beyond gland size, the pelvic floor physiology behind why Kegel exercises genuinely improve urinary control, and which natural interventions have the strongest randomised trial evidence. Natural ways to shrink prostate symptoms are real and meaningful — when combined with medical monitoring and an understanding of when escalation to pharmacological treatment or surgery is appropriate.
What BPH Actually Is — The Prostate Biology You Need to Understand
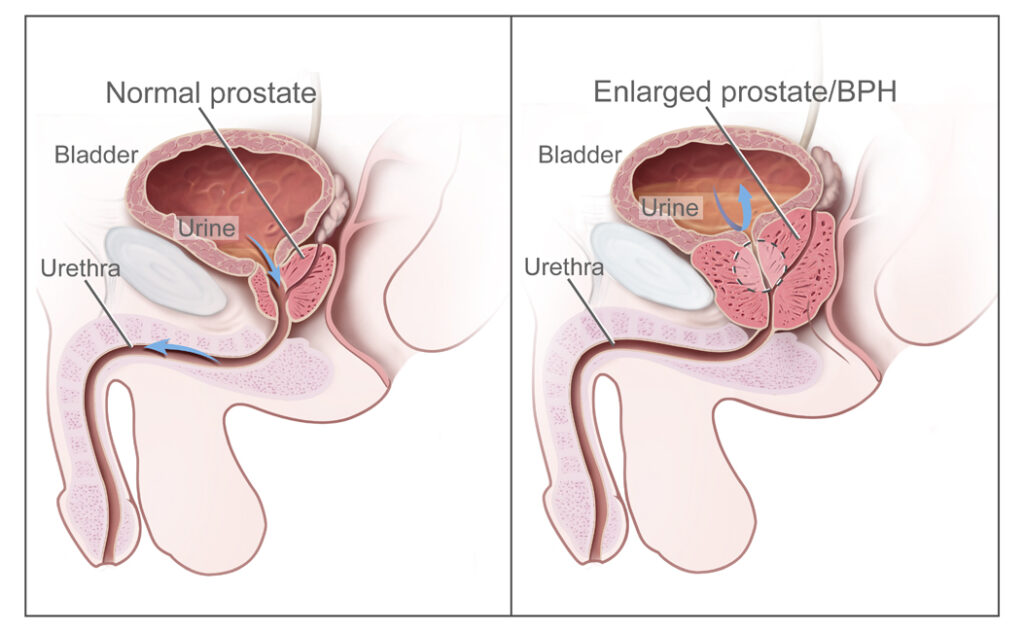
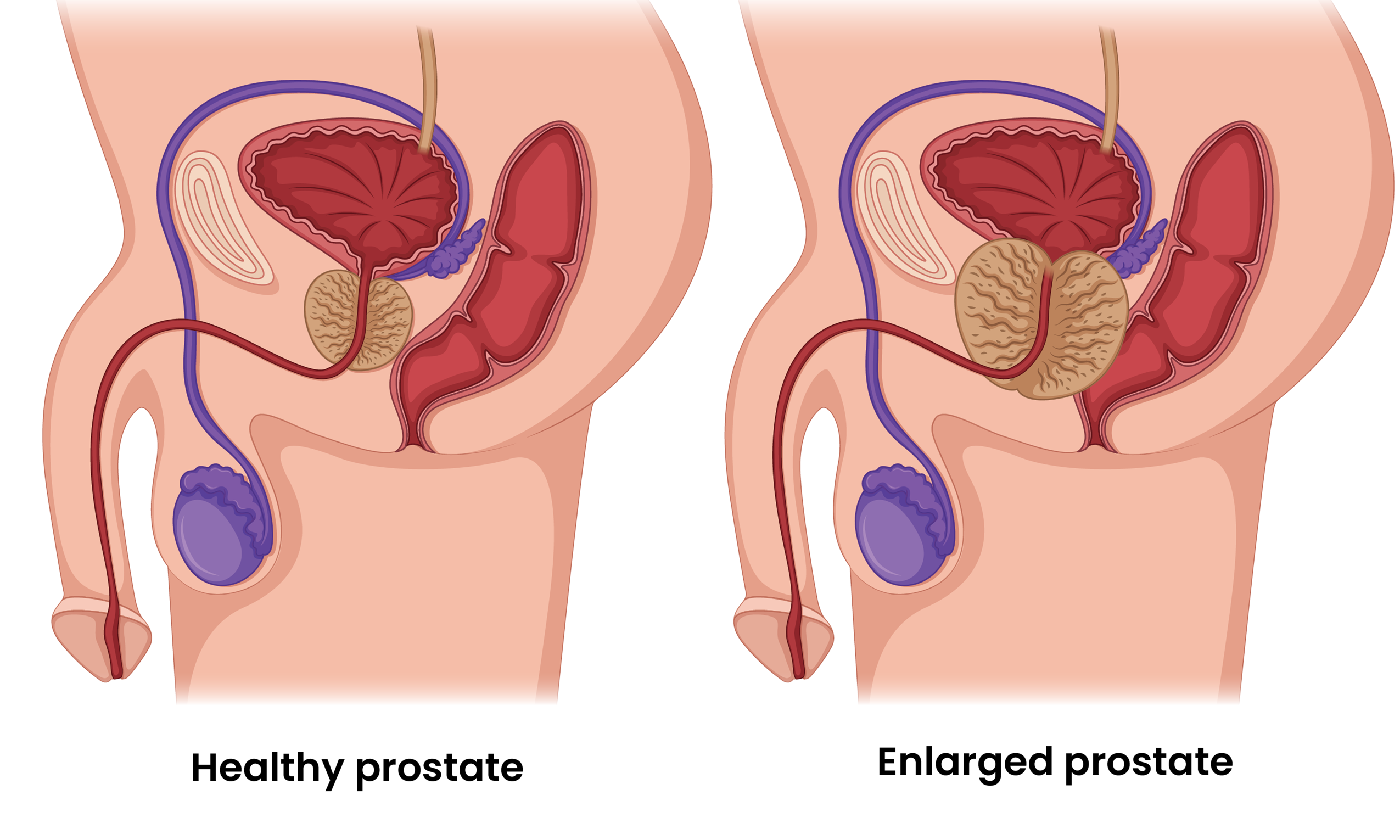
The prostate gland — a walnut-sized gland at the base of the bladder — surrounds the urethra (the tube through which urine exits the bladder). In BPH, the glandular and stromal cells of the prostate proliferate in the central transition zone, directly compressing the urethra and obstructing urinary outflow. This is the mechanical component of BPH. But there is a second, equally important component: smooth muscle tone in the bladder neck and prostate, mediated by alpha-1 adrenergic receptors — which is why alpha-blockers (tamsulosin) work so quickly and effectively even when prostate size has not changed.
Driver 1 — DHT-mediated prostatic growth: Testosterone is converted to dihydrotestosterone (DHT) by the enzyme 5-alpha reductase within prostate cells. DHT is approximately 5x more potent than testosterone at androgen receptors and is the primary hormonal driver of prostatic cell proliferation. As men age, DHT accumulates in the prostate even as circulating testosterone declines — creating a progressively androgenic prostate environment. Natural interventions targeting this pathway: saw palmetto (5-alpha reductase inhibition — same mechanism as finasteride), beta-sitosterol (androgen receptor modulation), zinc (5-alpha reductase cofactor regulation), and lycopene (androgen receptor gene expression reduction).
Driver 2 — Chronic prostatic inflammation: Emerging research positions prostatic inflammation as equally important to DHT in driving BPH progression. Infiltrating lymphocytes, macrophages, and elevated interleukins (particularly IL-17, IL-8, and TNF-α) in the prostate stimulate stromal cell growth independently of androgens. This explains why men with similar DHT levels and prostate sizes have vastly different symptom burdens — the inflammatory component drives the sensory and functional symptoms (urgency, frequency, incomplete emptying) more than the gland size itself. Natural anti-inflammatory interventions (omega-3s, lycopene, turmeric, green tea catechins) address this mechanism directly.
BPH Symptoms and Severity — Using the IPSS to Know Where You Stand
BPH produces lower urinary tract symptoms (LUTS) — a cluster of storage and voiding symptoms that progressively worsen with gland enlargement and inflammation. Understanding symptom severity objectively is important for tracking whether natural interventions are producing improvement.
Voiding symptoms (obstructive): Hesitancy (difficulty initiating urination — waiting for urine to start), weak or intermittent stream, straining (needing abdominal pressure to urinate), and prolonged urination time.
Storage symptoms (irritative): Frequency (urinating more than 8 times in 24 hours), urgency (sudden strong urge difficult to defer), and nocturia (waking 2+ times per night to urinate — the most sleep-disruptive BPH symptom).
Post-micturition symptoms: Sensation of incomplete emptying (residual urine feeling), and post-void dribbling (leakage after finishing).
10 Evidence-Backed Natural Ways to Support Prostate Health and Reduce BPH Symptoms
Lycopene is a carotenoid antioxidant found in highest concentrations in tomatoes, watermelon, and pink guava. It has the most robust epidemiological evidence of any dietary compound for prostate health — a 2004 meta-analysis published in Cancer, Epidemiology, Biomarkers and Prevention found that high lycopene intake was associated with an 11% reduction in prostate cancer risk overall, and 19% reduction in advanced prostate cancer specifically. For BPH specifically, lycopene reduces the expression of androgen receptor-regulated genes that drive prostatic cell proliferation, and acts as a potent quencher of reactive oxygen species in the oxidative-stress-heavy prostatic environment.
The bioavailability rule is critical and frequently missed: lycopene from raw tomatoes has low bioavailability (~4–7%) because it is embedded in cellular matrix. Cooking releases lycopene from cells and converts it from the cis to trans isomer, increasing bioavailability by 3–4 fold. Adding fat (cooking in oil) further increases absorption through the lymphatic route. Tomato sauce, tomato-based curry, rasam, and cooked tomato sabzi provide dramatically more bioavailable lycopene than raw tomatoes. Watermelon is the notable exception — its lycopene is highly bioavailable raw (higher water content disrupts cellular matrix). Pink guava provides lycopene comparable to tomatoes.
Pumpkin seeds (kaddu ke beej) are among the most evidence-supported natural interventions for BPH symptoms specifically. A 2019 randomised controlled trial published in Complementary Medicine Research found that pumpkin seed oil significantly reduced IPSS scores and nocturia (night-time urination frequency) in men with BPH compared to placebo over 12 weeks. An earlier 2014 randomised trial found similar results, with significant improvements in urinary flow rate and residual urine volume.
The mechanisms are multiple: pumpkin seeds are exceptionally rich in phytosterols (particularly beta-sitosterol) that modulate DHT-mediated prostatic growth; cucurbitin — a unique amino acid in pumpkin seeds — relaxes the detrusor (bladder wall) muscle, reducing urgency and frequency symptoms; delta-7-sterols in pumpkin seeds inhibit 5-alpha reductase, reducing DHT production; and pumpkin seeds are among the richest dietary sources of zinc — the mineral most highly concentrated in the healthy prostate and critically important for prostate immune function and cell integrity.
Beta-sitosterol is a plant sterol found in pumpkin seeds, sesame seeds, flaxseed, and various plant oils. It has the most robust clinical evidence of any natural compound for BPH symptom relief. A 1999 meta-analysis in the British Journal of Urology International reviewed four randomised, double-blind, placebo-controlled trials and found that beta-sitosterol significantly improved IPSS scores, increased peak urinary flow rate, and reduced residual post-void urine volume compared to placebo. The effect size was clinically meaningful — not just statistically significant.
The mechanism of beta-sitosterol in BPH is dual: structural similarity to cholesterol allows it to compete with cholesterol for absorption and incorporation into prostatic cell membranes, disrupting the pro-proliferative lipid rafts that support DHT receptor signalling; and beta-sitosterol directly inhibits 5-alpha reductase type 2 (the isoform preferentially expressed in the prostate and the primary target of the pharmaceutical finasteride). This pharmacological overlap with finasteride’s mechanism explains why beta-sitosterol produces meaningful BPH symptom improvement in clinical trials.
The healthy prostate has the highest zinc concentration of any organ in the human body — approximately 200mg/kg, compared to 20–30mg/kg in most other tissues. Zinc plays multiple critical roles in prostatic function: it inhibits 5-alpha reductase (reducing DHT production), promotes apoptosis (programmed cell death) of abnormal prostatic cells, supports the immune cells that patrol the prostate for early-stage malignant transformation, and maintains the structural integrity of the prostatic epithelium.
Studies consistently show that zinc concentrations in the prostate decline significantly with BPH and even more dramatically with prostate cancer — the loss of zinc accumulation in the malignant prostate is one of the most consistent biochemical features of prostate cancer. This has led to clinical investigation of zinc supplementation for prostate conditions. A 2011 study found that adequate zinc intake was inversely associated with prostate cancer risk. However, the relationship between zinc and prostate is complex: high-dose supplemental zinc (>100mg daily) has been associated with INCREASED prostate cancer risk in some studies — dietary zinc from food sources is far safer than high-dose supplementation and remains the recommended approach.
Green tea’s epigallocatechin gallate (EGCG) is among the most studied plant compounds in prostate health research — with both anti-BPH and prostate cancer-preventive mechanisms. For BPH specifically, EGCG reduces prostatic inflammation by inhibiting NF-kB activation (reducing pro-inflammatory cytokine production in prostatic macrophages and lymphocytes), and directly inhibits prostatic smooth muscle proliferation through EGFR (epidermal growth factor receptor) inhibition — addressing the stromal component of BPH growth. A 2017 systematic review found that green tea consumption was significantly associated with lower prostate cancer incidence — with the strongest evidence in Japanese populations where green tea consumption is highest globally.
A 2009 randomised trial found that green tea catechin supplementation (600mg/day for 1 year) significantly reduced IPSS scores and improved quality of life in men with BPH compared to placebo. The anti-inflammatory mechanism is particularly relevant for the symptom component of BPH — the urgency, frequency, and pelvic discomfort that correlate more with prostatic inflammation than with gland size.
Physical activity is one of the most consistently evidence-backed modifiable risk factors for BPH. A 2015 meta-analysis including 43,083 men found that higher physical activity was significantly associated with lower BPH risk and lower LUTS severity — with a dose-response relationship suggesting more exercise produces greater prostate benefit. The mechanisms are systemic and multiple: exercise reduces circulating insulin and IGF-1 (both of which stimulate prostatic cell proliferation), reduces systemic inflammation, reduces sympathetic nervous system tone (alpha-1 adrenergic receptor activation increases prostatic smooth muscle tone — exercise-induced reduction in sympathetic tone relaxes this smooth muscle and improves flow), and maintains testosterone/oestrogen balance that affects prostatic growth signalling.
Practically: physically active men have lower IPSS scores, better urinary flow rates, and lower rates of acute urinary retention than sedentary men — independent of prostate size and age. Walking 3+ hours weekly is associated with 25% lower BPH progression risk. Swimming and cycling are both beneficial — though cycling on a narrow seat increases perineal pressure and may worsen prostate symptoms, particularly in men already symptomatic. A wider, padded seat mitigates this.
⚗️ Meta-analysis 2015: 43,083 men — higher activity = lower BPH risk | Walking 3+hrs/week: 25% lower BPH progression | Reduced sympathetic tone → smooth muscle relaxationKegel exercises — voluntary contractions of the pelvic floor muscles (pubococcygeus muscle group) — are among the most evidence-backed non-pharmacological interventions for BPH-related urinary symptoms. They do not reduce prostate size but directly address the functional consequences of BPH: improved pelvic floor tone reduces urgency (by voluntarily suppressing the detrusor contraction), reduces urinary frequency (by improving voluntary control over voiding timing), reduces post-void dribbling (by milking residual urine from the bulbar urethra), and improves post-operative urinary function for men who undergo prostate procedures.
A 2005 randomised trial found that pelvic floor muscle training significantly reduced IPSS scores in men with LUTS from BPH — with improvements in both storage and voiding symptoms. The training effect — like any muscle training — requires consistency over 6–12 weeks before significant improvement is measurable, but the improvement is sustainable with ongoing practice.
The inflammatory component of BPH is increasingly recognised as a primary driver of symptom severity — particularly the storage symptoms (urgency, frequency) that correlate more with prostatic inflammation than with anatomical gland size. Curcumin — the active compound in turmeric — is among the most potent natural NF-kB inhibitors identified in pharmacological research, directly reducing the pro-inflammatory cytokine cascade (IL-17, IL-8, TNF-α) that drives BPH stromal growth and sensory symptoms.
Multiple in vitro and animal studies confirm curcumin’s direct anti-proliferative activity against prostate cells — inhibiting AR (androgen receptor) signalling, reducing PSA secretion, and inducing apoptosis in prostate cancer cell lines. Human clinical data in BPH specifically is limited but emerging — a 2016 study found curcumin significantly reduced prostate inflammation biomarkers and PSA in men with elevated PSA levels. The black pepper rule applies critically here: curcumin bioavailability is approximately 1% without piperine; adding black pepper increases this by 2,000%, making every haldi preparation pharmacologically relevant only when black pepper is included. For more on turmeric’s mechanisms: Health Benefits of Turmeric
The relationship between metabolic syndrome and BPH is among the strongest epidemiological associations in urology. Abdominal obesity, insulin resistance, high triglycerides, and high blood pressure — individually and collectively — significantly increase BPH risk and symptom severity. The mechanisms: adipose tissue (body fat) is an active oestrogen-producing endocrine organ, and excess oestrogen relative to testosterone creates a DHT-amplifying hormonal environment in the prostate; insulin resistance increases prostatic IGF-1 (insulin-like growth factor-1) stimulation of cell proliferation; chronic inflammation from metabolic syndrome adds to the prostatic inflammatory burden; and sympathetic nervous system overactivation (common in metabolic syndrome) increases alpha-1 adrenergic prostatic smooth muscle tone.
A 2006 study found that each unit increase in BMI was associated with significantly higher IPSS scores. Weight loss in overweight men with BPH produces measurable improvement in LUTS — not through prostate size reduction but through reduction in the metabolic and inflammatory drivers. For Indian men specifically — given the high prevalence of metabolic syndrome, abdominal obesity at lower BMI (TOFI pattern), and insulin resistance — addressing metabolic health is likely one of the highest-leverage interventions for prostate symptom management. Read more: Lower Blood Sugar Naturally: 10 Proven Ways
⚗️ BMI increase → higher IPSS scores | Adipose tissue oestrogen + IGF-1 prostatic proliferation | Weight loss → measurable LUTS improvementBehavioural modifications — sometimes called bladder training — are among the most evidence-backed non-pharmacological interventions for BPH storage symptoms (frequency, urgency, nocturia) and are recommended as first-line therapy in international urological guidelines for mild-moderate BPH. They do not change the prostate but directly address the learned and conditioned bladder behaviours that develop in response to BPH symptoms and independently worsen quality of life.
Key behavioural strategies: Timed voiding (urinating on a schedule every 2–3 hours regardless of urge, gradually lengthening the interval to 3–4 hours — trains the bladder to hold larger volumes); urge suppression (when urgency occurs, stand still or sit down, contract pelvic floor muscles 5 times rapidly to abort the urgency reflex, then walk calmly to the toilet — rather than rushing which worsens urgency); fluid management (adequate hydration during the day — 1.5–2 litres by 5pm — but significantly reducing fluid intake after 6pm to reduce nocturia; avoiding caffeine and alcohol which are bladder irritants); and avoiding prolonged sitting (perineal pressure worsens prostatic congestion and urinary symptoms).
A 2006 systematic review found that bladder training significantly reduced urgency episodes, frequency, and nocturia in men with LUTS from BPH — with improvements comparable to alpha-blocker medication in mild-moderate disease. These interventions have no side effects and can be combined with all natural and medical approaches.
Indian Foods for Prostate Health — Complete Reference Table
| Indian Food | Key Active Compound(s) | Prostate Benefit | Best Form | Evidence Level |
|---|---|---|---|---|
| Tomato (cooked) | Lycopene | Anti-proliferative, androgen receptor suppression, antioxidant | Cooked in oil (curry, rasam, sabzi) — 3–5x more bioavailable than raw | Strong (meta-analysis) |
| Pumpkin seeds (kaddu ke beej) | Beta-sitosterol, cucurbitin, zinc, delta-7-sterols | IPSS reduction, nocturia improvement, bladder relaxation | Raw or dry-roasted, 30g daily | Strong (multiple RCTs) |
| Til (sesame seeds) | Beta-sitosterol, zinc, lignans | 5-alpha reductase inhibition, androgen modulation | Til ladoo, til chutney, til in cooking | Moderate (phytosterol research) |
| Watermelon | Lycopene (highly bioavailable raw) | Anti-proliferative, antioxidant | Fresh fruit — excellent raw lycopene bioavailability | Moderate (lycopene epidemiology) |
| Green tea | EGCG (epigallocatechin gallate) | NF-kB anti-inflammatory, EGFR inhibition, anti-proliferative | 2–3 cups daily, brewed at 75°C not boiling | Moderate–Strong (RCT + SR) |
| Turmeric + black pepper | Curcumin + piperine | NF-kB inhibition, AR signalling suppression, PSA reduction | Haldi doodh daily, in all cooking with black pepper | Moderate (clinical + in vitro) |
| Flaxseed (alsi) | Lignans, omega-3 ALA, beta-sitosterol | Anti-androgenic (lignans converted to enterolignans), omega-3 anti-inflammatory | Ground flaxseed in roti, smoothie, or curd (1 tbsp daily) | Moderate (cohort + clinical) |
| Cruciferous vegetables (broccoli, cauliflower, cabbage) | Sulforaphane, indole-3-carbinol (I3C) | I3C modulates oestrogen metabolism, sulforaphane anti-proliferative in prostate cells | Lightly cooked (not overboiled — preserves sulforaphane) | Moderate (epidemiological + cell studies) |
| Walnuts (akhrot) | Omega-3 ALA, gamma-tocopherol, polyphenols | Anti-inflammatory, androgen pathway modulation | 5–7 walnuts daily as snack | Moderate (cohort studies) |
| Pink guava (amrood) | Lycopene, Vitamin C, quercetin | Lycopene anti-proliferative + Vitamin C antioxidant for prostate mucosa | Fresh fruit, in season | Moderate (lycopene content) |
Prostate Health Myths vs. Facts — Common Indian Misconceptions
“Prostate problems only affect old men. I’m under 50 and don’t need to worry.”
BPH symptoms can begin in the 40s, and prostate cancer — the second most common cancer in Indian men — is increasingly diagnosed in men under 55. Preventive dietary and lifestyle measures (lycopene, zinc, exercise, metabolic health) are most effective when started early. Men with a family history of prostate cancer should discuss PSA screening with their doctor from age 40 onward.
“Urinary symptoms in men are just a normal part of ageing — not worth discussing with a doctor.”
While BPH is common, urinary symptoms are never “just normal ageing” — they are treatable, manageable, and sometimes indicative of more serious conditions (prostate cancer, bladder pathology, urinary tract infection). Unmanaged severe BPH can lead to acute urinary retention, bladder damage, kidney complications, and urinary tract infections. Every man over 45 with urinary symptoms should have a medical evaluation.
“Sexual activity worsens an enlarged prostate.”
The opposite is more likely true. Regular ejaculation reduces prostatic congestion by clearing accumulated secretions from the glandular ducts. A 2016 study found that men who ejaculated more frequently had significantly lower prostate cancer risk. There is no evidence that sexual activity worsens BPH — and some evidence it may reduce prostatic stasis that contributes to inflammation.
“If I have an enlarged prostate, I will definitely need surgery eventually.”
Most men with BPH never require surgery. The majority are managed with lifestyle changes, natural interventions, and/or medication (alpha-blockers or 5-alpha reductase inhibitors) with excellent symptom control. Surgery (TURP or laser procedures) is indicated for severe refractory symptoms, acute urinary retention, recurrent infections, or bladder/kidney damage from chronic obstruction — a minority of BPH cases. Early intervention with lifestyle and natural approaches reduces the likelihood of progression to surgical intervention.
When to Consider Medical Treatment — Understanding Your Options
Natural interventions are most appropriate for mild BPH (IPSS 0–7) and as adjuncts to medical management for moderate BPH (IPSS 8–19). For men with IPSS scores above 15, quality-of-life significantly impacted, or progressively worsening symptoms — medical consultation is important, and the following conventional options are safe, effective, and frequently necessary.
Alpha-blockers (tamsulosin, alfuzosin, silodosin): Relax prostatic smooth muscle by blocking alpha-1 adrenergic receptors. Work rapidly (within days). Improve flow and reduce symptoms without affecting prostate size. First-line medication for moderate-severe BPH. Side effects: postural hypotension (blood pressure drop on standing), retrograde ejaculation (semen enters bladder during orgasm — harmless but startling).
5-alpha reductase inhibitors (finasteride, dutasteride): Block DHT production from testosterone, reducing prostate size by 20–30% over 6+ months. Best for men with demonstrably large prostates (>40ml volume). Take 6–12 months to show full benefit. Reduce long-term BPH progression risk. Side effects: reduced libido, erectile dysfunction (in a minority of men).
Combination therapy: Alpha-blocker + 5-ARI produces superior outcomes for men with large prostates and moderate-severe symptoms (as shown in the MTOPS and CombAT trials).
Minimally invasive and surgical options: TURP (transurethral resection of the prostate) — gold standard surgical approach with excellent symptom outcomes. Laser prostatectomy, UROLIFT, Rezum (water vapour therapy) — newer procedures with lower side effect profiles. Reserved for severe or refractory cases, or when complications (retention, infection, kidney damage) have developed.
Frequently Asked Questions About Natural Ways to Shrink Prostate
BPH symptoms include: frequent urination (more than 8 times/24 hours), urgency (sudden strong urge difficult to defer), nocturia (waking 2+ times nightly to urinate), weak or slow urinary stream, hesitancy (difficulty starting), straining to urinate, and sensation of incomplete bladder emptying. Symptom severity is assessed by IPSS: 0–7 mild (lifestyle management), 8–19 moderate (medical evaluation recommended), 20–35 severe (urologist referral urgently indicated).
Natural interventions produce modest anatomical volume change. What they significantly achieve: reduced symptom severity (IPSS improvement), improved urinary flow, reduced prostatic inflammation (which drives most symptoms), and slowed DHT-mediated growth progression. Beta-sitosterol, pumpkin seed oil, and saw palmetto have RCT evidence for symptom improvement. Pharmaceutical 5-alpha reductase inhibitors (finasteride, dutasteride) produce 20–30% volume reduction — but require physician prescription and have side effects. Natural interventions are most appropriate for mild-moderate BPH symptom management alongside medical monitoring.
Best Indian foods for prostate health: cooked tomato in oil (lycopene — 3–5x more bioavailable than raw), pumpkin seeds 30g daily (beta-sitosterol + cucurbitin + zinc + RCT evidence for IPSS improvement), til/sesame seeds (beta-sitosterol + zinc), watermelon (raw lycopene), green tea 2–3 cups daily (EGCG anti-inflammatory + anti-proliferative), turmeric with black pepper (NF-kB inhibition), flaxseed (lignans + omega-3), cruciferous vegetables (sulforaphane), walnuts (omega-3 + gamma-tocopherol), and pink guava (lycopene + Vitamin C).
The evidence for saw palmetto is mixed — earlier smaller RCTs showed benefit, but a 2011 Cochrane review of 30 trials found it not superior to placebo for most outcomes. The strongest natural BPH evidence is currently for beta-sitosterol (BJUI meta-analysis), pumpkin seed oil (2019 Korean RCT), and lifestyle interventions. Saw palmetto is safe with minimal side effects and may benefit some men, but should not be the sole reliance for moderate-severe symptoms. Medical evaluation remains important regardless of natural approach chosen.
See a doctor if you are 45+ with any urinary symptoms, have acute urinary retention (complete inability to urinate — emergency), blood in urine, pain with urination, IPSS score above 8, or symptoms significantly affecting quality of life. Men over 50 (or 40 with family history) should discuss PSA screening — prostate cancer and BPH can coexist and present similarly. Never delay medical evaluation based solely on natural management.
The best exercises for prostate health: regular aerobic exercise (brisk walking, swimming — 30 minutes most days; reduces IGF-1, insulin resistance, and sympathetic tone that drive BPH), and Kegel exercises (pelvic floor contractions — 3 sets of 10 daily; reduces urgency, frequency, and post-void dribbling through muscular urinary control). Avoid: narrow bicycle seats without perineal relief cut-out (increases prostatic pressure). A 2015 meta-analysis confirmed physically active men have significantly lower BPH risk and symptom scores than sedentary men.
Related Articles You’ll Love
90% of men over 85 have benign prostatic hyperplasia. The condition is universal in ageing men. What is not universal is the suffering — because the severity of BPH symptoms is not determined by gland size alone. The inflammatory burden, the metabolic health, the dietary choices, the physical activity, and the behavioural management all determine whether an enlarged prostate is a life-limiting condition or a minor inconvenience. Most of those factors are within your control.
The Indian kitchen has always known: cooked tomato, sesame, pumpkin, turmeric, and green tea. The science now explains exactly why these work — and how to use them most effectively. Start with your kitchen. Get evaluated by a doctor. Combine both.
Prostate health is built over decades of daily choices — not rescued by a single supplement. Start those choices today. 🌿Which prostate health strategy surprised you most — the lycopene bioavailability difference between raw and cooked tomato, the pumpkin seed RCT evidence, or the bladder training data outperforming medication for mild BPH? Share this with the men in your family who need the full picture. 👇
Sources & Further Reading
- Cancer Epidemiology, Biomarkers and Prevention (2004) — Lycopene Meta-Analysis: 11–19% Prostate Cancer Risk Reduction
- Complementary Medicine Research (2019) — Pumpkin Seed Oil RCT: IPSS Reduction and Nocturia Improvement in BPH
- British Journal of Urology International (1999) — Beta-Sitosterol Meta-Analysis: Significant IPSS + Flow + Residual Volume Improvement
- European Urology (2015) — Physical Activity and BPH/LUTS: Meta-Analysis of 43,083 Men
- Journal of Urology (2005) — Pelvic Floor Muscle Training RCT: Significant IPSS Reduction in Male LUTS
- Neurourology and Urodynamics (2006) — Bladder Training Systematic Review: Comparable to Alpha-Blockers for Mild-Moderate LUTS
- Phytotherapy Research (2009) — Green Tea Catechin Supplementation RCT: IPSS Reduction in BPH
- Molecular Nutrition and Food Research (2017) — Green Tea Systematic Review: Lower Prostate Cancer Incidence
- HerbeeLife — Health Benefits of Turmeric: NF-kB Anti-Inflammatory Mechanisms
- HerbeeLife — Natural Health & Ayurvedic Wellness
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Prostate conditions — including BPH and prostate cancer — require professional medical diagnosis and individualised management. Any man over 45 with urinary symptoms should seek evaluation. Never delay medical assessment in favour of natural management alone. Read full disclaimer →

