We approach this topic with the seriousness and warmth it demands — with the clinical detail that empowers women to advocate for themselves, and the compassion this subject always requires. Knowledge is the first step. Action is the second. Early detection is the outcome that changes everything.
What Breast Cancer Is — The Biology That Explains the Symptoms
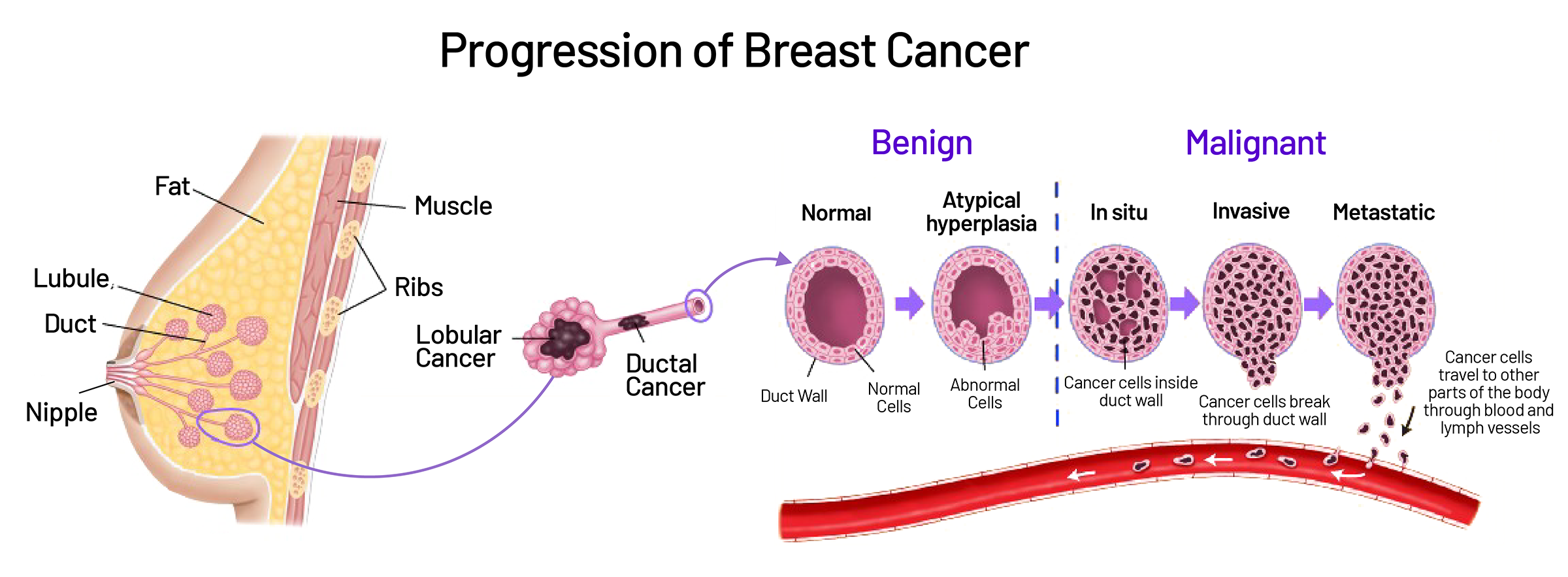
Breast cancer begins when cells in breast tissue undergo genetic mutations that cause them to grow and divide uncontrollably — forming a mass (tumour) and eventually spreading to surrounding tissue and distant organs (metastasis). Understanding where in the breast these mutations typically begin helps explain the symptoms they produce.
Ductal carcinoma in situ (DCIS): Abnormal cells confined within the milk ducts. Not yet invasive — the earliest stage. Often detected on mammogram (as micro-calcifications) before any palpable lump forms. With treatment, essentially 100% survival. This is the breast cancer that screening is designed to catch.
Invasive ductal carcinoma (IDC): The most common type (~80% of invasive breast cancers). Originates in milk ducts and invades surrounding breast tissue. Typically presents as a firm, irregular lump. Can spread to lymph nodes and beyond if not treated.
Invasive lobular carcinoma (ILC): Originates in milk-producing lobules. Accounts for ~10% of invasive breast cancers. More difficult to detect by mammogram and physical examination — it tends to spread in single file cells without forming a distinct mass, producing thickening rather than a lump.
Triple-negative breast cancer (TNBC): Lacks oestrogen receptors, progesterone receptors, and HER2 overexpression. More common in younger women and in Indian women (significantly higher proportion than in Western populations). More aggressive — grows faster, is harder to treat with targeted therapies, and more commonly presents at advanced stage. Strongly associated with BRCA1 mutations.
Inflammatory breast cancer (IBC): Rare but aggressive — presents with rapid breast swelling, redness, warmth, and skin thickening (peau d’orange) rather than a discrete lump. Often mistaken initially for a breast infection (mastitis). Requires urgent evaluation — any new breast redness and swelling that does not resolve with antibiotics within one week must be evaluated for IBC.
HER2-positive breast cancer: Overexpresses the HER2 protein — grows faster than hormone-receptor-positive cancers but responds specifically to targeted anti-HER2 therapies (trastuzumab/Herceptin) that have transformed outcomes.
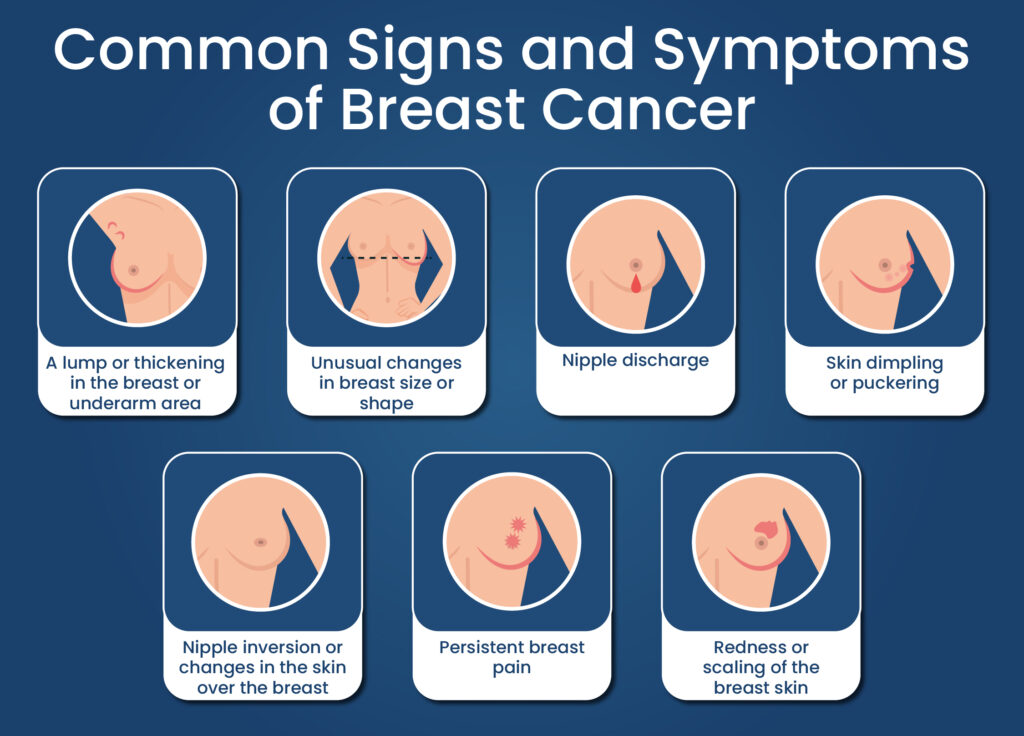
Breast Cancer Symptoms — The Complete Picture, Including What Most Guides Miss
The most important thing to know about breast cancer symptoms is this: early breast cancer is almost always asymptomatic. The cancers that are curable — Stage I DCIS and early invasive cancers — typically cause no pain, no discomfort, and no visible change. By the time a cancer produces noticeable symptoms, it has usually been present for months or years. This is why self-examination and screening are not supplementary to watching for symptoms — they are the primary detection strategy.
The absence of pain does not mean a lump is safe. Most early breast cancers are painless. In India, one of the most common reasons women delay seeking evaluation is the belief that a painless lump is not dangerous — and this belief costs lives. If you or someone you know has a new breast lump, skin change, nipple change, or axillary swelling — please seek medical evaluation within days, not months. The timeliness of that step is the difference between Stage I and Stage III.
Breast Cancer Causes and Risk Factors — What Raises the Risk and What You Can Change
Approximately 5–10% of all breast cancers are caused by inherited mutations in known high-risk genes — most significantly BRCA1 and BRCA2 (BReast CAncer genes 1 and 2). A woman with a BRCA1 mutation has approximately 55–72% lifetime risk of breast cancer (compared to approximately 12% in the general population). A BRCA2 mutation carrier has approximately 45–69% lifetime risk. Both mutations also significantly elevate ovarian cancer risk (BRCA1 ~44% lifetime risk, BRCA2 ~17%).
Other high-risk inherited mutations include TP53 (Li-Fraumeni syndrome), PTEN (Cowden syndrome), CDH1, PALB2, CHEK2, and ATM. A 2023 Lancet publication identified multiple novel breast cancer susceptibility loci through GWAS (genome-wide association studies), expanding the understanding of genetic risk beyond BRCA genes.
The India-specific genetic context: Specific BRCA founder mutations (recurring mutations carried in particular population groups due to a common ancestor) have been identified in Indian communities, including Ashkenazi-pattern mutations in certain South Indian populations. Genetic testing for BRCA mutations is increasingly available in India and recommended for: women with breast cancer diagnosed before 40, bilateral breast cancer, breast and ovarian cancer in the same woman, multiple first-degree relatives with breast/ovarian cancer, and male breast cancer. Family history of breast cancer — particularly in first-degree relatives (mother, sister, daughter) — is one of the strongest individual risk factors.
⚗️ BRCA1: 55–72% lifetime breast cancer risk | BRCA2: 45–69% | India-specific founder mutations identified | Genetic testing recommended for high-risk familiesOestrogen and progesterone drive the growth of hormone-receptor-positive breast cancers — which account for approximately 70% of all breast cancers. The duration and intensity of lifetime hormonal exposure are significant risk modulators. Factors that increase cumulative oestrogen exposure and associated risk: early menarche (before age 12), late menopause (after age 55), nulliparity (never having been pregnant), late age at first full-term pregnancy (after 35), hormone replacement therapy (HRT) — particularly combined oestrogen-progestogen HRT for more than 5 years in post-menopausal women, and oral contraceptive use (modest, reversible elevation in risk during and shortly after use).
Factors that reduce cumulative oestrogen exposure and associated risk: earlier first pregnancy, breastfeeding (each year of cumulative breastfeeding reduces lifetime breast cancer risk by 4.3% — the Lancet 2002 Collaborative Group analysis), earlier menopause, physical exercise (reduces circulating oestrogen through adipose tissue reduction), and maintaining healthy weight (adipose tissue is a significant post-menopausal oestrogen source). Read more about breastfeeding’s protective effect: Breastfeeding Benefits: The Complete Science Guide
⚗️ Oestrogen drives ~70% of breast cancers | Breastfeeding: 4.3% risk reduction per 12 months | Adipose tissue: post-menopausal oestrogen sourceBreast cancer incidence increases with age — the majority of cases in Western populations are diagnosed after 50. However, the age distribution in India differs significantly: Indian women develop breast cancer at younger ages (peak incidence in the 40–50 age decade), with a significant proportion of cases in women under 40. This younger age pattern is partly biological (higher proportion of hormone-receptor-negative, triple-negative breast cancers in younger women) and partly detection-related (younger women are less likely to be screened and more likely to present with advanced disease).
The India-specific implication: screening and awareness strategies cannot be calibrated for a post-50 target population as in some Western contexts. Indian women should begin breast self-examination at 20, clinical breast examination at 25–30, and discuss mammography timing with their doctor from 40 onward (or earlier with risk factors).
⚗️ Indian peak incidence: 40–50 (vs 60–65 in Western populations) | Higher proportion of aggressive subtypes in younger Indian womenApproximately 30% of breast cancer cases are attributable to modifiable lifestyle factors — representing a meaningful prevention opportunity. The evidence-backed modifiable risk factors:
Alcohol: Even moderate drinking (1 drink daily) increases breast cancer risk by approximately 7–10%. There is no established safe threshold for alcohol and breast cancer — risk increases with every unit consumed. The mechanism: alcohol elevates circulating oestrogen, impairs DNA repair mechanisms, and increases acetaldehyde (a direct carcinogen) exposure to breast cells. This is among the most robustly established dietary breast cancer risk factors.
Obesity and weight gain: Obesity after menopause is a significant breast cancer risk factor — adipose tissue is the primary post-menopausal oestrogen source, and higher fat mass means higher circulating oestrogen. Weight gain of 20kg or more in adulthood approximately doubles post-menopausal breast cancer risk. Abdominal obesity (central fat distribution) may carry additional risk through insulin resistance and IGF-1 elevation.
Physical inactivity: Regular physical activity consistently reduces breast cancer risk by approximately 20–30% across cohort studies — through oestrogen reduction, insulin sensitisation, immune function improvement, and direct anti-proliferative effects. 150 minutes of moderate aerobic activity weekly is the recommended target.
Smoking: Particularly in pre-menopausal women, smoking is associated with modestly elevated breast cancer risk — particularly with long duration and high pack-year exposure. The association is stronger for women who began smoking before their first pregnancy.
⚗️ Alcohol: 7–10% risk increase per drink/day | Post-menopausal obesity: doubles risk | Physical activity: 20–30% risk reductionDense breast tissue — where the breast contains more glandular and fibrous tissue relative to fat — is an independent breast cancer risk factor. Women with extremely dense breasts have approximately 4–5x higher breast cancer risk than women with mostly fatty breasts. Dense breast tissue also reduces mammogram sensitivity (cancers are harder to detect against a dense background), creating both higher risk and lower detection — a particularly challenging combination.
Previous breast biopsies showing atypical ductal hyperplasia (ADH) or lobular carcinoma in situ (LCIS) — non-malignant but pre-malignant proliferative conditions — elevate lifetime breast cancer risk by 4–5x and 8–10x respectively. Women with these findings require more frequent surveillance. A history of previous breast cancer significantly elevates the risk of a new primary cancer in either breast.
⚗️ Extremely dense breasts: 4–5x higher cancer risk + reduced mammogram sensitivity | ADH: 4–5x risk | LCIS: 8–10x riskPrevious chest or thoracic radiation — particularly during childhood or adolescence (as historically used for Hodgkin’s lymphoma treatment) — significantly elevates lifetime breast cancer risk. The breast tissue of young women is particularly sensitive to radiation-induced carcinogenesis. Modern radiation techniques have substantially reduced this risk, but women who received chest radiation before 30 require enhanced surveillance protocols.
Endocrine-disrupting chemicals (EDCs) — compounds that mimic or interfere with oestrogen and other hormones — are an area of growing research concern. Bisphenol A (BPA) from plastic containers, phthalates from plastics and personal care products, and organochlorine pesticides (DDT residues, which remain detectable in Indian women’s blood decades after agricultural application) all have experimental evidence for breast carcinogenesis through oestrogenic activity. For Indian women: minimising plastic food container use (particularly heating food in plastic), choosing BPA-free products, and washing fresh produce thoroughly are practical risk reduction steps supported by the precautionary principle.
⚗️ Chest radiation before 30: significant lifetime risk elevation | BPA/phthalates: endocrine disruption mechanism | Organochlorine pesticide residues in Indian women’s bloodHow to Do a Breast Self-Examination — The Step-by-Step Guide
Breast self-examination (BSE) is the foundation of breast awareness — not a replacement for clinical examination or mammography, but an essential complement that allows women to know their own breast tissue well enough to notice when something changes. Monthly BSE from the age of 20 is recommended.
When: 7–10 days after the start of your period — when breasts are least swollen and tender. Post-menopausal women should choose a fixed monthly date (e.g., the first day of each month).
Breast Cancer Screening — Who Should Be Screened, When, and With What
| Age / Risk Group | Recommended Screening | Frequency | Notes |
|---|---|---|---|
| Women 20–39 (average risk) | Monthly breast self-examination (BSE) + clinical breast examination (CBE) by a healthcare provider | BSE monthly, CBE every 1–3 years | Know your baseline. Any new finding prompts imaging. Mammography not routinely recommended but may be done for clinical indications. |
| Women 40–49 (average risk) | BSE + CBE + mammography discussion with doctor | BSE monthly, CBE + mammogram annually | Indian guidelines increasingly support beginning mammography at 40. Dense breasts may need supplemental ultrasound. Discuss with your doctor for personalised timing. |
| Women 50–69 (average risk) | BSE + CBE + mammogram | BSE monthly, CBE + mammogram annually or biannually | Most breast cancer diagnoses in India occur in this decade. This is the highest-priority screening window for average-risk Indian women. |
| Women 70+ (average risk) | BSE + CBE + mammogram | Discuss with doctor — based on health status and life expectancy | Screening should continue as long as the woman is in good health and would pursue treatment if cancer were found. |
| High-risk women — Family history of breast/ovarian cancer, known BRCA mutation, previous atypical biopsy | Annual mammogram + annual MRI + CBE every 6 months + BRCA genetic counselling and testing | More intensive — as directed by specialist | Begin screening 10 years earlier than youngest affected family member’s diagnosis age (minimum age 25). Referral to breast cancer genetics clinic is recommended. |
| Prior chest radiation before age 30 (e.g., for Hodgkin’s lymphoma) | Annual mammogram + annual MRI beginning 8 years after radiation (minimum age 25) | Annual | High-risk group requiring enhanced surveillance. Discuss with oncologist. |
Breast Cancer Myths vs. Facts — Misconceptions That Cost Lives in India
“My lump doesn’t hurt, so it’s probably not cancer.”
Pain is the least reliable indicator of breast cancer. The vast majority of early breast cancers are entirely painless. A painless lump is not reassuring — it still requires prompt medical evaluation. This belief causes women to self-reassure and delay evaluation for months or years. Please do not wait for pain to appear before seeking assessment of a new breast lump.
“Breast cancer only happens to women over 60. I’m too young to worry.”
Indian women develop breast cancer a decade earlier than Western women — the peak incidence is in the 40–50 age group. A significant proportion of Indian breast cancer cases occur in women under 40. Breast self-examination should begin at 20. Any age woman with a new breast finding deserves evaluation, not dismissal based on age.
“No one in my family has had breast cancer, so I’m at low risk.”
Approximately 85% of women who develop breast cancer have no family history. Family history significantly elevates risk — but its absence does not confer protection. Breast cancer can and does arise in women with no family history through acquired genetic mutations driven by age, hormonal factors, and lifestyle. All women need breast awareness regardless of family history.
“If I find something, I’m scared of what they’ll find — so I’d rather not know.”
This fear — deeply human and completely understandable — costs more lives in India than almost any other factor in breast cancer outcomes. Stage I breast cancer has 5-year survival approaching 99%. Stage IV falls below 28%. The cancer does not wait for the courage to seek evaluation. Early detection is the most powerful tool available — and it exists precisely for the moment before fear becomes reality.
“Breast cancer is always a death sentence.”
Stage I breast cancer treated appropriately has 5-year survival approaching 99% and 10-year survival above 90%. Even Stage II has 5-year survival above 85%. Modern targeted therapies — including hormone therapies, HER2-targeted agents, CDK4/6 inhibitors, PARP inhibitors for BRCA carriers, and immunotherapy — have transformed outcomes across all stages. Breast cancer, detected early, is among the most treatable cancers. The narrative of breast cancer as a death sentence is outdated and prevents women from seeking life-saving early detection.
“Wearing an underwire bra or using deodorant causes breast cancer.”
Neither claim has any scientific evidence. The underwire bra-lymph flow theory and the deodorant-aluminium-breast cancer hypothesis have both been specifically studied and found to have no causal relationship with breast cancer. These myths persist online and in informal health communication — they distract from evidence-based risk factors (alcohol, obesity, physical inactivity, hormone exposure) and evidence-based protective behaviours (BSE, screening, breastfeeding).
When to Seek Medical Evaluation — And How to Advocate for Yourself
Any new lump or thickening in the breast or armpit — regardless of whether it is painful, soft, or small. The only way to determine whether a breast lump is benign or malignant is through imaging and (if indicated) biopsy. Self-diagnosis is not adequate.
Skin changes: dimpling, puckering, peau d’orange, redness, or unusual texture that is new.
Nipple changes: new inversion, discharge that is spontaneous/unilateral/bloody/clear, persistent scaling or crusting of the nipple skin.
Breast or axillary swelling — including swelling of the entire breast, particularly with redness and warmth.
Persistent focal breast pain — pain that is non-cyclical, localised, and persistent beyond 2–3 menstrual cycles.
Any change from your normal breast baseline — if something is different from last month, have it checked.
If you visit a doctor and feel dismissed: You are entitled to ask specifically — “I would like a clinical breast examination and imaging given this new finding.” You are entitled to a second opinion. You are your own most important advocate. Do not accept dismissal of a breast finding you are concerned about without appropriate investigation.
Frequently Asked Questions About Breast Cancer Symptoms and Causes
Early breast cancer is almost always asymptomatic — which is why screening is critical. When symptoms do appear: a new painless lump or thickening in the breast or armpit (most common); skin dimpling, puckering, or peau d’orange (orange peel texture); new nipple inversion; spontaneous, unilateral, bloody, or clear nipple discharge; breast size or shape change; skin redness or warmth; and axillary lymph node swelling. Painless lumps are not reassuring — most early breast cancers do not cause pain. Any new breast finding deserves prompt medical evaluation.
Monthly BSE, 7–10 days after your period. Three positions: (1) In the shower — use three-finger pads in circular motions with three pressure levels across the entire breast and armpit. (2) In front of a mirror — visual inspection with arms at sides, raised, and hands pressed on hips — look for dimpling, skin changes, asymmetry. (3) Lying down — towel under shoulder, examine opposite breast in vertical strips with three pressure levels. Any new finding (lump, thickening, skin change, nipple change) — seek medical evaluation within days.
Breast cancer results from genetic mutations in breast cells allowing uncontrolled growth. Causes include: inherited mutations (BRCA1/BRCA2 — 5–10% of cases), prolonged hormonal exposure (early menarche, late menopause, HRT, nulliparity), age (risk increases with age — but Indian women present younger than Western populations), lifestyle factors (alcohol, obesity, physical inactivity, smoking), previous atypical breast biopsy, dense breast tissue, and previous chest radiation. Approximately 85% of breast cancers have no family history — most are not inherited.
BSE monthly from age 20. Clinical breast examination (CBE) by a healthcare provider from age 20–25, every 1–3 years in the 20s and 30s, annually from 40 onward. Mammography: discuss with your doctor from age 40 — some guidelines recommend annually from 40, others from 45–50. High-risk women (family history, BRCA mutation, prior atypical biopsy) should begin enhanced surveillance earlier. Indian women should not wait for symptoms — early stage breast cancer is typically asymptomatic.
Physical examination alone cannot reliably distinguish benign from malignant — imaging and biopsy are required. Features suggesting benign: smooth margins, mobile, soft or cystic, bilateral, cyclically varying, may be tender. Features raising cancer concern: irregular margins, fixed (not freely mobile), hard, unilateral, non-cyclical, typically painless. Critical point: the assumption that a soft, mobile, or tender lump is benign is one of the most dangerous delays in breast cancer diagnosis. Every new lump needs evaluation.
Breast cancer is India’s most common cancer in women since 2022, with over 178,000 new cases annually. Indian women present younger (40–50 average vs 60–65 in the West), with more aggressive tumour subtypes, and at more advanced stages — primarily because of lower screening rates and delayed presentation. India-specific concerns include younger age of onset, high proportion of triple-negative breast cancer, specific BRCA founder mutations in some Indian communities, and cultural barriers to breast examination and discussion. Five-year survival in India is lower than in Western countries primarily because of later stage at detection.
Related Articles You’ll Love
The gap between breast cancer survival rates in India and in Western countries is not primarily a gap in treatment technology or medical expertise. It is a gap in the stage at which the cancer is found. Stage I breast cancer detected through regular screening and awareness is almost completely curable. Stage III breast cancer presenting because of a lump that has been growing for two years while a woman waited to see if it would go away is a vastly harder battle.
The most powerful thing any woman reading this can do right now: check your breasts tonight. Know what is normal for you. Schedule a clinical breast examination if you haven’t had one. And share this guide with every woman you love.
Early detection is not just a medical recommendation. It is the most important act of self-care a woman can perform. 🌸Which piece of information surprised you most — the 99% Stage I survival rate, the fact that most early breast cancers are painless, or that Indian women develop breast cancer a decade younger than Western women? Share this with every woman in your family — the knowledge in this guide could be the most important gift you give them this year. 👇
Sources & Further Reading
- The Lancet (2002) — Collaborative Group: Breastfeeding and Breast Cancer Risk — 4.3% Reduction per 12 Months
- Nature Genetics (2013) — BRCA1/BRCA2 Lifetime Risk Estimates: Meta-Analysis
- GLOBOCAN 2022 — India Cancer Incidence: Breast Cancer as #1 Female Cancer
- The Lancet Oncology (2015) — Triple-Negative Breast Cancer: Higher Prevalence in South Asian Women
- Journal of Clinical Oncology (2017) — Breast Density and Cancer Risk: Population-Based Study
- JAMA Internal Medicine (2015) — Alcohol and Breast Cancer Risk: Dose-Response Meta-Analysis
- National Cancer Institute — Breast Cancer Screening: Evidence Summary
- HerbeeLife — Breastfeeding Benefits: Including the 50% Lifetime Breast Cancer Risk Reduction
- HerbeeLife — Natural Health & Ayurvedic Wellness
Disclaimer: This content is for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Any breast findings or symptoms must be evaluated by a qualified healthcare provider. Please consult a doctor for personalised screening and risk assessment. Read full disclaimer →

