Why 2am–4am Specifically? The Sleep Architecture You Need to Know
The 2am–4am window is not arbitrary. It sits at the transition point between two fundamentally different halves of the sleep night — and understanding this architecture explains why waking here feels so specific.
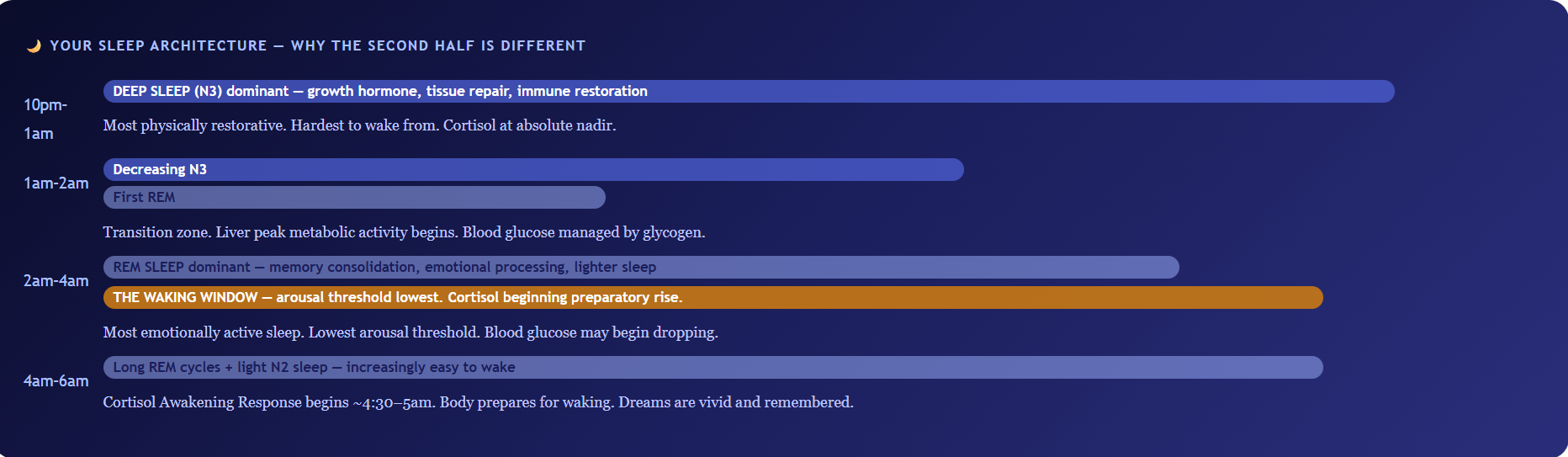
The 2am–4am window is where deep sleep has largely been completed and the brain has shifted to a lighter, REM-dominant mode. The arousal threshold — how much stimulation is needed to wake you — is at its lowest. This means that any internal signal that would be slept through during deep sleep now has enough amplitude to produce full waking. The signals that commonly reach this threshold in this window: a cortisol spike, a blood glucose drop, an adrenaline release, a racing mind, or an airway obstruction. Understanding which signal is waking you is the entire diagnosis.
The Causes — What Your Body Is Telling You at 3am
📈
Cortisol follows a precise daily rhythm — lowest at midnight, beginning its preparatory rise at approximately 4–5am, peaking 30–45 minutes after waking (the Cortisol Awakening Response). This morning rise serves a purpose: it mobilises glucose and prepares the immune system for the day ahead. In people under chronic stress — a description that applies to an estimated 80% of Indian urban adults — the HPA axis is dysregulated. The cortisol rhythm flattens and shifts earlier. Instead of beginning its rise at 4–5am, it begins at 1–2am. This premature rise is activating rather than quietly preparatory — it produces wakefulness, mental activation, and the inability to return to sleep that characterises stress-driven 3am waking.
The physiological cascade: elevated early-morning cortisol activates the locus coeruleus (the brain’s alertness centre), increases noradrenaline, raises heart rate and blood pressure, and shifts brain activity from the slow-wave oscillations of sleep toward the high-frequency beta waves of wakefulness. The person wakes fully — not groggily, but with the alertness of someone who has just been started. They lie in the dark, unable to understand why they cannot sleep, while their brain chemistry says they should be awake.

⚗️ Chronic stress → HPA axis dysrhythmia → premature cortisol rise 1–2am → locus coeruleus activation → full wakefulness | Affects ~80% chronically stressed Indian adults
🌿 What to Do — Cortisol-Driven 3am Waking
- Ashwagandha 300–600mg at bedtime:Withanolides inhibit premature HPA axis activation — the cortisol rise is delayed back to its appropriate 4–5am timing. A 2012 RCT found ashwagandha reduced serum cortisol by 27.9% over 60 days. See: How to Reduce Cortisol Naturally
- Magnesium glycinate 300–400mg at bedtime:NMDA antagonism and GABA-A agonism reduce the neural excitability that cortisol exploits to produce early waking.
- Fixed consistent wake time:The single most evidence-backed intervention for circadian rhythm normalisation — waking at the same time 7 days/week anchors the cortisol awakening response to the correct morning hour, gradually pulling the premature rise back.
- 10 minutes of 4-7-8 breathing before bed:Inhale 4 counts, hold 7, exhale 8 — activates vagal tone, reduces overnight HPA reactivity. Reduces nocturnal cortisol pulse frequency.
- If you wake at 3am — do not check your phone.Screen light at 3am triggers a cortisol spike, confirms wakefulness to the circadian system, and makes returning to sleep harder. Eyes closed, diaphragmatic breathing.
🩸
The brain is the most metabolically demanding organ per gram of tissue in the body — and unlike muscle, it cannot store glucose or use fatty acids directly as fuel. It requires a continuous supply of blood glucose. During sleep, this supply comes from the liver’s glycogen stores, which release glucose steadily overnight through a process called glycogenolysis. The liver stores approximately 100–120g of glycogen — enough for approximately 8–12 hours of fasting. If dinner was eaten early (7pm, common in many Indian households), glycogen stores may deplete around 3–5am. When blood glucose begins to fall, the body triggers an emergency response: adrenaline (epinephrine) and cortisol are released to stimulate gluconeogenesis (converting stored protein and fat to glucose). Both are alerting hormones. The result: the person wakes with a pounding heart, a slight sweat, mild anxiety, and an awareness of hunger — at precisely 2–4am.
This cause is particularly prevalent in Indian adults who eat dinner early, those following low-carbohydrate diets (reduced glycogen stores), people with reactive hypoglycaemia (blood sugar drops more rapidly after meals), and diabetics whose overnight insulin activity may cause glucose to fall below comfortable levels. The distinctive clue: waking with hunger, mild sweating, heart pounding, and feeling significantly better after eating something — even a glass of warm milk restores glucose and allows return to sleep.
⚗️ Liver glycogen depletes 8–12h post-dinner → adrenaline + cortisol release → arousal | Early dinner = 3am glycogen nadir | Adrenaline = pounding heart + anxiety-like symptoms
🌿 What to Do — Blood Sugar Waking
- Small, low-GI bedtime snack:A handful of walnuts (5–7) or 1 tbsp almond/peanut butter — the combination of fat and protein provides slow-release glucose substrate, maintaining overnight blood glucose without causing an insulin spike that could trigger reactive hypoglycaemia. Alternatively: 1 small piece of dark chocolate (fat + minimal sugar).
- Move dinner later if too early:A 7:30–8pm dinner reduces the overnight fasting window to 10–11 hours at the 6am wake time — typically within glycogen capacity for most people.
- Protein-rich dinner:Gluconeogenic amino acids (from protein) provide an additional glucose substrate during the overnight fast — reducing the rate of glycogen depletion.
- For diabetics on insulin:Nocturnal hypoglycaemia requires medical management — discuss with your endocrinologist. A bedtime snack protocol needs to be agreed with your diabetes team.
- If you wake at 3am and suspect this cause:Drink a glass of warm milk (lactose provides glucose, protein provides gluconeogenic substrate). If you return to sleep within 20 minutes — blood sugar waking is confirmed.
🫁
Both Traditional Chinese Medicine and modern hepatic chronobiology converge on the 1am–3am window as the liver’s most metabolically active period. In TCM, this corresponds to the liver’s organ clock slot — a time when liver Qi processes emotions (particularly unresolved anger and frustration) and the liver performs its blood-cleaning function. In modern biochemistry: hepatic gluconeogenesis (glucose production) is highest in the early morning hours; liver enzyme activity for Phase 1 and Phase 2 detoxification peaks in the early morning; and the liver’s circadian clock genes (BMAL1, CLOCK, PER2) drive a metabolic programme specifically timed to this window. When the liver is congested — from excess alcohol, fatty liver disease, heavy late dinners, or toxic load — this peak metabolic activity may produce enough systemic metabolic signalling to produce arousal.
The India-specific context: non-alcoholic fatty liver disease (NAFLD) affects approximately 38% of urban Indians — making it the most common liver condition in the country. A congested or inflamed liver may produce more inflammatory cytokines (IL-6, TNF-α) during its overnight activity peak — cytokines that are independently associated with sleep disruption. Additionally, a large late Indian dinner (the traditional heavy post-work meal, commonly eaten at 9–10pm in urban families) puts significant digestive and hepatic processing demand on the liver that extends into the 1–3am window — potentially disrupting the quieter sleep that this window should produce.
⚗️ Liver circadian clock: BMAL1, PER2 drive peak gluconeogenesis + detoxification 1–3am | NAFLD affects 38% urban Indians | Inflammatory cytokines from congested liver disrupt sleep architecture
🌿 What to Do — Liver-Related Waking
- Finish dinner by 7:30–8pm maximum:Allowing 3–4 hours between dinner and sleep means liver processing of the meal completes before sleep architecture reaches the 1–3am window. Late dinners (10pm) guarantee peak liver activity coincides with peak sleep vulnerability.
- Keep dinner light in the evening:The heaviest meal should be lunch — not dinner. This is the most evidence-backed and Ayurvedically consistent advice for liver-related sleep disruption.
- Reduce or eliminate alcohol:Alcohol is directly hepatotoxic and disrupts sleep architecture specifically — it may appear to induce sleep but consistently produces early waking as the liver processes acetaldehyde during the 1–3am window.
- Triphala at bedtime (½ tsp in warm water):Amalaki’s antioxidants protect hepatic mitochondria; haritaki’s chebulic acids support liver Phase 2 conjugation; bibhitaki’s ellagic acid has hepatoprotective effects. Triphala supports liver function without stimulating it, potentially reducing the metabolic arousal from liver activity. See: Natural Remedies for Constipation — Triphala Guide
- Reduce dietary fat and sugar:Both directly contribute to NAFLD — reducing the hepatic congestion that makes overnight liver activity more disruptive to sleep.
💭
REM sleep is the brain’s emotional processing and memory consolidation phase — it is when the hippocampus replays emotional experiences and the prefrontal cortex (in a low-noradrenaline environment) reprocesses them with reduced emotional charge. This is why sleep literally helps emotional pain feel better the next morning. But in anxious individuals, the emotional material being processed during REM is not comfortably contained in sleep — it surfaces into wakefulness. The 3am waking with anxious thoughts is not the anxiety causing bad sleep; it is sleep attempting to process unresolved anxiety and the process becoming conscious.
This is why the thoughts at 3am feel more catastrophic than they would in the afternoon — the prefrontal cortex is at its most depleted during this early morning window (reduced noradrenaline from long sleep), and the amygdala (the brain’s threat-detection system) has higher relative influence. Problems feel unsolvable. Fears feel realer. The same worry that could be rationally managed at 2pm feels overwhelming at 3am — because the rational override system is partially offline. Understanding this helps: the thoughts at 3am are not more true than the thoughts you have in the afternoon. They are simply processed by a brain at reduced executive capacity.
⚗️ REM sleep: emotional memory reprocessing in low-noradrenaline environment | 3am prefrontal cortex most depleted → amygdala relatively dominant → catastrophising | Thoughts feel more threatening at 3am than 3pm
🌿 What to Do — Anxiety-Driven 3am Waking
- The “worry window” technique:Schedule 15 minutes in the afternoon (not evening) as your designated worry time — write down every worry and a next step for each. This externalises the anxiety from the REM processing queue. Research confirms “worry scheduling” significantly reduces rumination-driven night waking.
- If you wake at 3am with thoughts: don’t resist them.Resistance amplifies anxiety. Instead: acknowledge the thought (“I am thinking about the EMI payment again — that thought is visiting”), label it without judgment, and return attention to breathing. Cognitive defusion reduces rumination duration.
- The 4-7-8 breathing when awake:Inhale 4 counts through nose, hold 7 counts, exhale 8 counts through mouth. Repeat 4–6 cycles. This activates the vagus nerve, reducing amygdala reactivity and lowering cortisol enough to allow sleep re-entry.
- Ashwagandha + brahmi at bedtime:Both reduce GABAergic tone for the nervous system, reducing the amplitude of anxious arousal during the sleep-anxiety interface.
- Evening digital detox:No news, social media, or work email after 9pm — preventing the anxiety loading that the REM system then has to process at 3am.
🕐
The circadian rhythm — the body’s internal 24-hour clock — determines when sleep pressure peaks, when cortisol rises, and when the brain transitions between sleep stages. This clock is calibrated primarily by light exposure and sleep timing consistency. “Social jet lag” — the pattern of sleeping late Friday-Saturday and waking early for work Monday-Friday — continuously misaligns the circadian clock, producing a state similar to mild chronic jet lag. When the circadian clock is misaligned, sleep architecture becomes disorganised: the first half of the night may be acceptable (driven by sleep pressure — the accumulation of adenosine during waking hours), but the second half — which is circadian-dependent — becomes fragmented. The result: early waking at 2–4am as the misaligned clock attempts to begin its morning arousal sequence at the wrong biological time.
This is particularly prevalent in Indian urban professionals who work late, use screens until 1–2am on weekends, then struggle to wake at 6am for the work week — and then wonder why their sleep quality is poor Sunday through Thursday nights. The fix requires circadian discipline more than any supplement or herbal remedy — consistent sleep and wake times are the primary treatment for circadian-driven early waking.
⚗️ Social jet lag: circadian clock misalignment = fragmented second-half sleep | Circadian arousal sequence begins at wrong biological time → early waking | Adenosine pressure drives first half; circadian drives second half
🌿 What to Do — Circadian Disruption Waking
- Fixed wake time 7 days/week — no exceptions:The wake time is the master anchor of the circadian clock. Even if you sleep late on Saturday, wake at the same time. Accept the tiredness — sleep pressure will ensure better sleep the following night.
- Morning bright light within 30 minutes of waking:10–15 minutes of outdoor light (or a 10,000 lux light therapy lamp in winter months) anchors the circadian clock with precision. This is the most powerful single circadian re-setter available.
- Screens off by 10pm consistently:Blue light suppresses melatonin and signals “daytime” to the circadian clock — pushing sleep timing later and making the morning arousal sequence arrive prematurely.
- Melatonin 0.5–1mg at consistent bedtime:Low-dose melatonin (not 5–10mg — these doses are far above physiological) at a consistent time helps re-anchor the circadian phase. The dose matters — 0.5mg is more effective than 5mg for circadian resetting.
😮💨
Obstructive sleep apnoea (OSA) — the repeated partial or complete collapse of the upper airway during sleep, producing oxygen desaturation and arousal — is significantly underdiagnosed in India. An estimated 13–32% of Indian adults have OSA; only a fraction are diagnosed. Sleep apnoea is most severe during REM sleep — the muscle paralysis that characterises REM (atonia) extends to the upper airway muscles, making the airway more collapsible. Since REM sleep concentrates in the 2am–5am window, OSA-related arousals are most likely in this window — making sleep apnoea a specific cause of 3am waking that is frequently misattributed to anxiety or cortisol.
The Indian risk factors for OSA are significant: the increasingly prevalent metabolic syndrome (central obesity), high prevalence of retrognathia (smaller jawline anatomy in South Asian populations), neck circumference increase with weight gain, and nasal congestion from allergic rhinitis (ubiquitous in Indian cities). OSA is not just a sleep problem — untreated OSA significantly increases cardiovascular risk, worsens hypertension, drives insulin resistance, and is associated with depression. If there is any possibility that 3am waking is associated with snoring, waking with a dry mouth, gasping, or witnessed breathing pauses — OSA evaluation is urgent.
⚗️ REM atonia → upper airway collapse → oxygen desaturation → arousal | 2–5am REM concentration = peak OSA arousal window | 13–32% Indian adults affected — most undiagnosed
🌿 What to Do — Sleep Apnoea Waking
- Medical evaluation first — this is non-negotiable:A polysomnography (sleep study) or home sleep apnoea test (HSAT) confirms diagnosis. OSA requires treatment — CPAP therapy is the gold standard. No natural remedy adequately treats moderate-to-severe OSA.
- Weight loss:Every 10% reduction in body weight reduces OSA severity by approximately 30% in overweight individuals. For moderate OSA in overweight people, weight loss alone can resolve or significantly reduce the condition.
- Side sleeping:Positional OSA (worse when sleeping on the back) responds to sleeping on the side. A tennis ball sewn into the back of a sleep shirt is an old-fashioned but effective side-sleeping enforcer.
- Nasal congestion management:Allergic rhinitis treatment (nasal corticosteroid spray — discuss with ENT) significantly reduces OSA severity in many patients by improving nasal airflow.
- Avoid alcohol and sedatives:Both relax upper airway muscles further — significantly worsening OSA events.
✨
Magnesium deficiency reduces the brain’s NMDA receptor block — producing neural hyperexcitability that lowers the arousal threshold during the vulnerable 2–4am window. The transition from deep to light sleep that occurs around 2am normally happens without full waking. With a hyperexcitable nervous system from magnesium deficiency, this transition produces a full arousal rather than a seamless stage change. Additionally, magnesium deficiency is the most common cause of nocturnal leg cramps — the intense calf muscle spasms (from Ca²⁺-ATPase pump failure) that wake people from sleep at precisely this window when muscle tone is lowest and cramps most easily triggered. Restless legs syndrome — the urge to move legs during rest — peaks in the early morning hours and is associated with magnesium and iron deficiency.
Beyond magnesium: other physical causes that produce 2–4am waking include acid reflux (lying flat allows stomach acid to reflux into the oesophagus; the supine position used during sleep combined with the relaxation of the lower oesophageal sphincter during REM makes 3am the peak GERD symptom window); back or joint pain (pain threshold is lower during light sleep); nocturia (the need to urinate, particularly in men with enlarged prostates or people with uncontrolled diabetes); and cold or hot temperatures disrupting sleep continuity. For more on magnesium: What Magnesium Deficiency Does to Your Body
⚗️ Mg deficiency: reduced NMDA block → lower arousal threshold | Ca²⁺-ATPase failure → nocturnal leg cramps | GERD: supine position + REM sphincter relaxation = 3am peak reflux
🌿 What to Do — Physical Cause Waking
- Magnesium glycinate 300–400mg at bedtime:Addresses leg cramps (Ca²⁺-ATPase restoration), restless legs (dopaminergic pathway support), and neural hyperexcitability simultaneously. Effects within 5–10 days.
- GERD:Head-of-bed elevation (raise the head of the bed by 15–20cm using blocks — this is more effective than extra pillows which cause neck flexion that worsens reflux); avoid eating within 3 hours of sleep; reduce coffee, alcohol, and spicy dinner foods. See the ash gourd juice morning protocol for gastric mucosa protection: Ash Gourd Benefits
- Room temperature:18–20°C is the optimal sleep temperature for most adults. A cooler room dramatically improves sleep continuity — a fan (even in air-conditioned rooms) prevents the body temperature rise that produces 3am waking in warm Indian nights.
- Nocturia:Reduce fluid intake after 7pm (particularly diuretic beverages — chai, coffee, alcohol). For men with prostate symptoms: saw palmetto discussion with urologist. For diabetics: improved blood glucose control reduces osmotic diuresis.
The Complete 3am Waking Fix — Before Bed and What to Do When You Wake
🌙 Before Bed — Building the Conditions for Unbroken Sleep
- Fixed bedtime and wake time — 7 days/week, no exceptions. The foundation of circadian discipline.
- Dinner by 7:30–8pm, light and protein-inclusive — prevents both blood sugar drop and liver overload.
- Screens off by 9:30–10pm — prevents melatonin suppression and anxiety loading from news/social media.
- Ashwagandha 300mg + Magnesium glycinate 300mg — 60–90 minutes before bed. The most evidence-backed natural sleep support combination.
- 10 minutes 4-7-8 breathing — reduces HPA axis reactivity and overnight cortisol pulse frequency.
- “Worry window” journalling — 15 minutes in the afternoon to externalise anxiety from the REM queue.
- Room temperature 18–20°C — physically enables sleep continuity through the 2–4am vulnerable window.
- Small bedtime snack if dinner was early — 5–7 walnuts or 1 tbsp nut butter for blood glucose stability.
🌅 If You Wake at 3am — The Return-to-Sleep Protocol
- Do not check the phone or clock. Light triggers cortisol; knowing the time increases arousal. Eyes stay closed.
- Begin 4-7-8 breathing immediately: Inhale 4 counts, hold 7, exhale 8. Repeat 6–8 cycles. This is the fastest route back to sleep for cortisol or anxiety waking.
- Body scan from feet to head: Systematically relax each muscle group. This interrupts the cognitive loop and redirects attention from thoughts to body sensation.
- If hungry or anxious with heart pounding: Get up quietly, drink 100ml warm milk with ¼ tsp ashwagandha powder. Return to bed. Do not turn on full lights.
- If thoughts are racing: Label them neutrally (“thinking is happening”) — do not engage, do not resist. Return to breathing.
- If awake for 20+ minutes: Get up. Sit in dim light. Read a physical book (not a screen). Return to bed when drowsy. Do not lie awake fighting sleeplessness — this creates anxiety-about-sleep that worsens the pattern.
- Do not compensate with a nap the next day — it reduces sleep pressure for the following night, perpetuating the cycle.
What Ayurveda Says About 2am–4am Waking — And Why It Aligns With Modern Biology
3am Waking Myths vs. Facts
“Waking at 3am every night means you have insomnia.”
Waking once briefly in the 2–4am window is within the range of normal sleep — human sleep evolved as a biphasic pattern (two main sleep periods) and brief awakenings are normal, particularly in the lighter second half of the night. “Insomnia” is defined clinically by difficulty falling asleep AND staying asleep AND the waking being associated with daytime impairment AND occurring at least 3 nights per week for 3+ months. Occasional 3am waking without significant distress or daytime impairment is common and not pathological.
“If you wake at 3am, you should try harder to go back to sleep.”
Effortful sleep is an oxymoron — trying hard to sleep produces performance anxiety about sleep, which activates the arousal system and makes sleep less likely. The counterintuitive truth: passive wakefulness (lying quietly with no effort to sleep, simply resting) is more effective than active sleep-effort. If awake for more than 20 minutes, getting up briefly (stimulus control therapy) is more effective than staying in bed awake — the bed should be associated with sleep, not with anxious wakefulness.
“Alcohol before bed helps prevent 3am waking.”
Alcohol sedates the first half of the night by suppressing REM sleep — but as the liver metabolises it (producing acetaldehyde, which is arousing), REM sleep rebounds in the second half. Alcohol reliably fragments the 2–5am window — producing more waking, more vivid dreams, and less restful sleep. The apparent initial sleep-induction is replaced by significant second-half disruption. Alcohol is one of the most reliable causes of 3am waking.
“Melatonin in high doses will fix early waking.”
Melatonin is a circadian signal, not a sedative — it tells the body what time it is, not to go to sleep. High doses (5–10mg, commonly sold in India) do not improve sleep quality and can produce next-day grogginess, rebound insomnia, and hormone disruption with regular use. For circadian re-anchoring: 0.5–1mg melatonin at consistent bedtime is effective; higher doses are not more effective and produce more side effects. For sleep quality: magnesium glycinate has substantially more evidence than high-dose melatonin.
⚠️ See a Doctor for Sleep Evaluation If:
Early waking is accompanied by snoring, gasping, or dry mouth on waking (sleep apnoea — requires polysomnography). Night waking with chest pain, palpitations, or shortness of breath (cardiac evaluation needed). Waking with severe anxiety or panic attacks (clinical anxiety disorder — cognitive behavioural therapy for insomnia, CBT-I, is the gold-standard treatment). Early morning waking as the primary symptom of a low mood that persists throughout the day (waking early — especially earlier than desired — is a classic symptom of clinical depression; requires psychiatric evaluation). Sleep disruption that has persisted for more than 3 months despite consistent application of the lifestyle interventions above — chronic insomnia requires specialist sleep medicine assessment. Sleepiness during the day so severe it affects work, driving, or daily function — possibly narcolepsy or severe sleep apnoea.
Frequently Asked Questions
The most common causes in Indian adults: (1) Premature cortisol rise from chronic stress — HPA axis dysregulation shifts the cortisol morning rise from 4–5am to 1–2am, producing early alerting. (2) Blood sugar drop — if dinner was early, liver glycogen depletes around 3–5am, triggering an adrenaline + cortisol release that wakes you. (3) Anxiety and rumination — REM sleep processes emotional memories; unresolved anxiety surfaces during this lighter sleep window. (4) Liver metabolic peak — congested liver (NAFLD, alcohol, late dinner) produces metabolic arousal during 1–3am peak activity. (5) Sleep apnoea — REM sleep concentrates in this window; OSA events produce most arousal here. Use the clue signatures from each cause to identify yours — the fix is cause-specific.
Very commonly, yes — but with an important nuance. The anxiety is not random; the 3am window is when the brain is in REM sleep (emotional memory processing), the prefrontal cortex is at its most depleted, and the arousal threshold is lowest. Unresolved worries are processed in this window and surface into wakefulness. The thoughts feel more catastrophic at 3am than they would at 3pm — because rational inhibition of the amygdala is reduced. Treatment: the “worry window” technique (scheduled afternoon worry time), ashwagandha and brahmi at bedtime, 4-7-8 breathing on waking, and digital detox from 9pm.
The 2am–6am window is Vata dosha time — governing movement, air, and nervous system activity. Waking here indicates Vata vitiation (excess light, mobile, nervous energy disturbing sleep). Ayurvedic management: abhyanga (warm sesame oil massage before bed — grounds Vata), ashwagandha + brahmi (reduce neural excitability = reduce Vata), warm milk with nutmeg (mild serotonergic sedation), early light dinner (prevents Pitta-liver cascade into Vata time), and being asleep before 10pm Kapha window. These recommendations align precisely with modern cortisol management, blood sugar stabilisation, and liver support principles.
Yes — this is nocturnal hypoglycaemia and is common in early-dinner Indians, people on low-carb diets, and diabetics on insulin. When liver glycogen depletes (7–9 hours after an early dinner), adrenaline + cortisol are released to restore blood glucose. Both produce arousal — heart pounding, mild sweat, anxiety-like feelings, hunger. Fix: a small bedtime snack of walnuts or nut butter maintains overnight blood glucose. If eating something at 3am reliably allows return to sleep — this is the cause. Diabetics: discuss nocturnal hypoglycaemia management with your endocrinologist.
Fix depends on cause. Universal interventions that help all causes: (1) Fixed wake time 7 days/week — the most powerful single circadian anchor. (2) Magnesium glycinate 300–400mg at bedtime — addresses cortisol dysrhythmia, neural hyperexcitability, leg cramps, and sleep quality simultaneously. (3) Ashwagandha 300–600mg at bedtime — specifically delays premature cortisol rise. (4) Dinner by 7:30–8pm, light, protein-inclusive — prevents blood sugar and liver causes. (5) Screens off by 10pm — prevents melatonin suppression and anxiety loading. (6) Room temperature 18–20°C. For the 3am waking itself: eyes closed, no phone, 4-7-8 breathing, body scan.
Related Articles You’ll Love
The 3am waking is not insomnia. It is not weakness. It is not your body betraying you in the middle of the night. It is a signal — from your cortisol rhythm, or your liver, or your blood glucose, or your nervous system, or your airway — that something specific is happening that needs attention. Each cause is identifiable. Each has a targeted fix. None requires a prescription or an extreme intervention.
Most people who consistently wake at 3am need three things: a fixed wake time to anchor their circadian rhythm, magnesium glycinate at bedtime to reduce neural hyperexcitability, and either ashwagandha (for cortisol) or a small bedtime snack (for blood sugar) to address their specific cause. That is genuinely all.
Tonight: phone away at 10pm. Magnesium glycinate with warm milk at 10:30. Fixed wake time tomorrow. Week by week, your 3am will get quieter. 🌙Which cause resonated with your 3am? The premature cortisol rise that wakes you fully alert with a racing mind, the blood sugar drop that wakes you hungry and heart-pounding, or the liver connection to the late Indian dinner? Share this with everyone who has sat in the dark at 3am wondering what is wrong with them. Nothing is wrong. Your body is just talking. 👇
Sources & Further Reading
- Sleep Medicine Reviews (2013) — Sleep Architecture in the Second Half of the Night: REM Dominance, Arousal Threshold, and Vulnerability to Waking
- Indian Journal of Psychological Medicine (2012) — Ashwagandha RCT: 27.9% Cortisol Reduction — HPA Axis Normalisation Mechanism
- Journal of Research in Medical Sciences (2012) — Magnesium Supplementation RCT: Significantly Improved Sleep Quality, Efficiency and Time in Insomniacs
- Journal of Clinical Sleep Medicine (2013) — Nocturnal Blood Sugar and Sleep Architecture: Hypoglycaemia-Induced Arousal Mechanism
- Sleep Medicine (2017) — Indian Obstructive Sleep Apnoea Prevalence: 13–32% of Adults; OSA Worst During REM Sleep
- Journal of Clinical Medicine (2018) — Liver Circadian Clock Genes (BMAL1, PER2): Peak Hepatic Metabolic Activity 1–3am and Sleep Architecture Interaction
- Behaviour Research and Therapy (2015) — Worry Scheduling (Designated Worry Time): Significantly Reduces Rumination and Night Waking in Anxious Insomnia
- HerbeeLife — Home Remedies for Better Sleep: The Complete Natural Guide
- HerbeeLife — Natural Health & Ayurvedic Wellness
Disclaimer: This content is for informational purposes only and does not constitute medical advice. Persistent sleep disturbance, particularly with daytime impairment, requires evaluation by a qualified healthcare provider. Sleep apnoea specifically requires medical diagnosis and treatment — it cannot be adequately managed with lifestyle measures alone. Read full disclaimer →

