Osteoarthritis is the most prevalent musculoskeletal disorder in the world — affecting an estimated 500 million people globally and representing the leading cause of chronic pain and physical disability in adults over 50. In India, the burden is particularly significant: a population-based study published in the Indian Journal of Rheumatology estimates that osteoarthritis affects approximately 15–20% of the Indian adult population, with knee osteoarthritis disproportionately affecting Indian women (who develop it earlier and more severely than their Western counterparts, partly due to prolonged floor-sitting, squatting postures in cooking and household work, and higher rates of Vitamin D deficiency).
Despite its prevalence, osteoarthritis is persistently misunderstood in two equally damaging directions: it is either accepted as an inevitable, unstoppable consequence of ageing that requires only pain management — or it is treated with unfounded optimism about “reversing” cartilage damage through unproven supplements and detoxes. Neither framework serves patients well. The accurate, evidence-based understanding is more nuanced and more empowering: osteoarthritis home remedies and evidence-based lifestyle interventions cannot reverse established cartilage loss, but they can significantly slow progression, substantially reduce pain and functional limitation, preserve joint function over years and decades, and in many cases provide better outcomes than pharmaceutical pain management without the associated side effect burden.
This guide covers the disease in the depth it deserves — the pathophysiology that explains why specific interventions work, the evidence for each approach, the Ayurvedic wisdom of Sandhivata management, a practical targeted exercise programme, and the nutritional strategies with the strongest joint health evidence.
Understanding Osteoarthritis — The Biology of Joint Degeneration
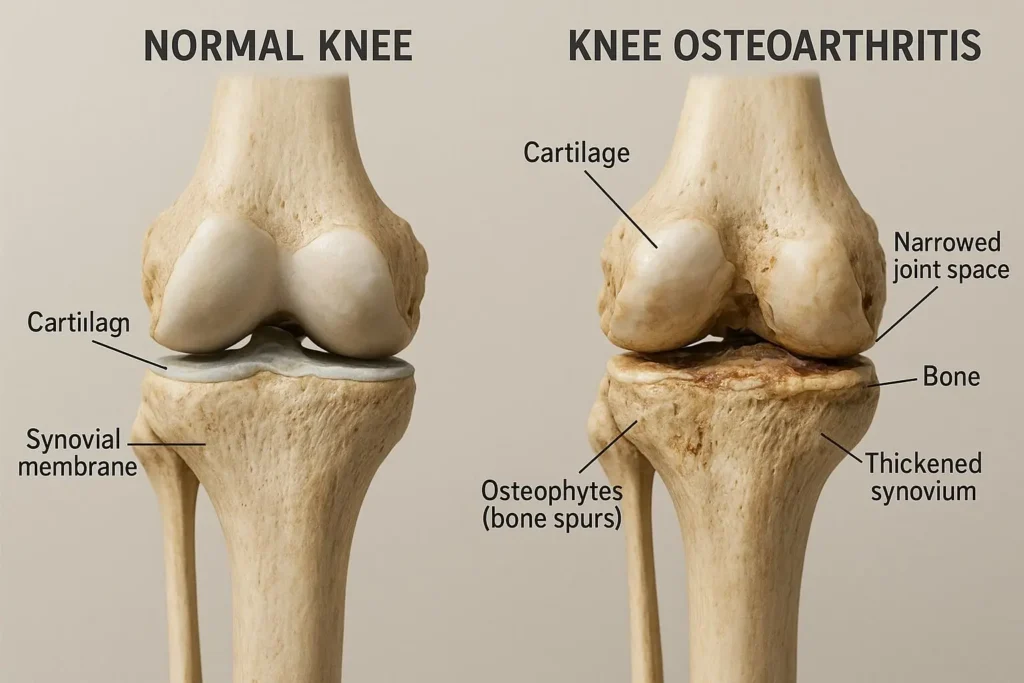
Osteoarthritis is not simply “wear and tear” — a description that implies the joint inevitably grinds down like a machine. It is a dynamic disease of the entire joint organ — involving articular cartilage, subchondral bone, synovium, periarticular muscles, ligaments, and joint capsule — driven by a complex interplay of mechanical, metabolic, and inflammatory factors.
Healthy articular cartilage is a remarkable tissue: avascular (without blood vessels), aneural (without nerve supply), and composed of a highly organised extracellular matrix of collagen (primarily type II) and proteoglycans (primarily aggrecan) maintained by chondrocytes — the cartilage cells. This matrix is continuously remodelled by the balance between anabolic processes (chondrocyte synthesis of new matrix components) and catabolic processes (matrix metalloproteinase and aggrecanase-mediated degradation). In osteoarthritis, this balance shifts toward net catabolism — driven by biomechanical stress, inflammatory cytokines (IL-1β and TNF-α from the inflamed synovium), and metabolic factors including obesity-associated adipokines that reach the joint via systemic circulation.
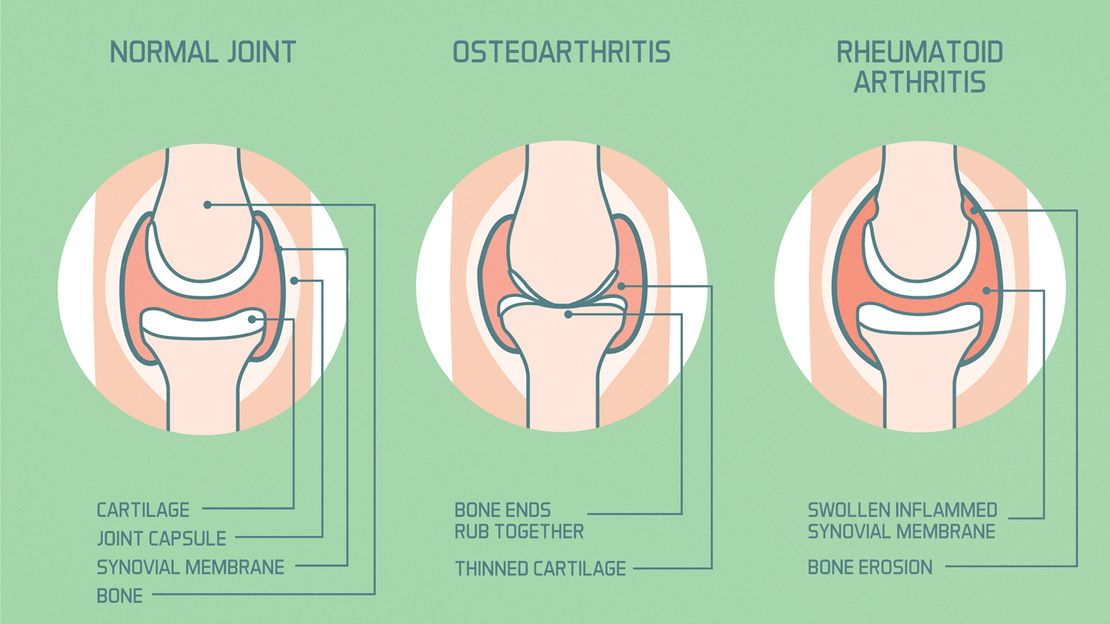
The result is progressive cartilage thinning and eventually full-thickness loss, sclerosis (hardening) and remodelling of the underlying subchondral bone (producing the typical X-ray findings of joint space narrowing, subchondral sclerosis, and osteophyte formation), and synovial inflammation (low-grade synovitis — not as dramatic as rheumatoid arthritis but clinically significant in driving pain and cytokine-mediated catabolic acceleration). The pain of osteoarthritis does not come from cartilage itself (which is aneural) but from the richly innervated structures surrounding it: the synovium, the joint capsule, periarticular ligaments, subchondral bone (which becomes exposed and stress-sensitive as cartilage is lost), and the periarticular muscles that develop pain secondary to protective spasm and fatigue.
Understanding this biology makes clear why the most effective osteoarthritis home remedies and interventions target: reduction of the inflammatory burden driving cytokine-mediated cartilage catabolism (anti-inflammatory diet, omega-3 supplementation, weight management), mechanical offloading of the affected joint (weight loss — the most powerful mechanical intervention available), muscle strengthening to improve joint mechanics and reduce peak contact stress, and pain management that does not impair function or accelerate joint damage.
Osteoarthritis Staging — What Grade Are Your Joints?
Osteoarthritis is staged using the Kellgren-Lawrence (K-L) radiological grading system, which assesses the degree of joint space narrowing, osteophyte formation, subchondral sclerosis, and bone deformity on plain X-ray:
Grade 0: No radiological features of osteoarthritis. Normal joint. Prevention-focused interventions are most impactful at this stage.
Grade 1 (Doubtful): Possible minimal osteophytes. Minimal or no joint space narrowing. Symptoms may be absent or mild. Conservative management and lifestyle modification are highly effective.
Grade 2 (Mild): Definite osteophytes. Possible joint space narrowing. Symptoms present but often mild-moderate. Conservative management with exercise, weight loss, and anti-inflammatory strategies produces excellent outcomes at this grade.
Grade 3 (Moderate): Multiple osteophytes, definite joint space narrowing, some sclerosis, possible bone deformity. Significant symptoms. Conservative management remains important, often supplemented with physiotherapy and judicious use of pain management. Intra-articular injections (corticosteroid or hyaluronic acid) may be appropriate at this stage.
Grade 4 (Severe): Large osteophytes, marked joint space narrowing, severe sclerosis, definite bone deformity. Significant functional limitation. When quality of life is severely impaired despite comprehensive non-surgical management, joint replacement is the appropriate intervention — producing excellent outcomes for knee and hip osteoarthritis.
Most people with symptomatic osteoarthritis are Grade 2–3 — the grades at which conservative management has the greatest impact on slowing progression and maintaining function.
12 Evidence-Based Osteoarthritis Home Remedies and Strategies
1. Weight Management — The Most Powerful Modifiable Osteoarthritis Intervention
Weight loss is the highest-impact single intervention for knee and hip osteoarthritis management — and the one most frequently underemphasised in favour of symptom-focused treatments. The biomechanical relationship between body weight and knee joint loading is not proportional: each kilogram of excess body weight translates to approximately 3–6 kilograms of additional compressive force through the knee joint during walking (the “lever arm effect” of gait mechanics). A 5kg weight loss therefore reduces knee joint loading by 15–30kg per step — multiplied across the thousands of steps per day, this produces enormous cumulative reduction in the mechanical stress that drives cartilage catabolism.
Clinical research confirms this dramatic effect: the IDEA trial (Intensive Diet and Exercise for Arthritis) published in JAMA found that intensive dietary weight loss plus exercise produced greater pain reduction and functional improvement in knee osteoarthritis than either diet or exercise alone — with 10% body weight loss producing outcomes superior to exercise alone that were comparable to intra-articular corticosteroid injections, without any adverse effects. Every unit of BMI reduction produces measurable reduction in knee osteoarthritis symptoms.
Beyond pure biomechanics, adipose tissue — particularly visceral fat — produces adipokines (leptin, adiponectin, resistin, visfatin) that directly promote synovial inflammation and cartilage catabolism through cytokine signalling. Weight loss reduces this metabolic inflammatory burden alongside the mechanical benefit, addressing osteoarthritis pathophysiology at multiple levels simultaneously. The dietary strategies for weight management covered in our weight loss diet vs exercise guide are directly applicable to osteoarthritis management as their most clinically significant benefit.
2. The Anti-Inflammatory Diet — Reducing the Cytokine Burden on Cartilage
The synovial inflammation that drives cytokine-mediated cartilage catabolism in osteoarthritis responds to the same anti-inflammatory dietary interventions that reduce systemic inflammation more broadly. The dietary pattern with the strongest evidence for joint health and osteoarthritis pain management combines: high omega-3 fatty acid intake (from fatty fish, walnuts, flaxseed), high antioxidant-rich plant foods (berries, leafy greens, colourful vegetables), adequate Vitamin C for collagen synthesis, and minimal refined carbohydrates, industrial seed oils, and ultra-processed foods that promote the chronic inflammatory state that worsens joint disease.
Omega-3 fatty acids deserve specific emphasis: EPA and DHA from marine sources directly reduce the production of inflammatory eicosanoids (prostaglandin E2, leukotriene B4) and inflammatory cytokines (TNF-α, IL-1β) — the same cytokines that directly degrade articular cartilage matrix in osteoarthritis. A meta-analysis of clinical trials found that omega-3 supplementation significantly reduced pain and morning stiffness in arthritic conditions. Fatty fish (sardines, mackerel, hilsa), walnuts, and ground flaxseed are the most accessible Indian dietary sources. The comprehensive framework is in our anti-inflammatory foods guide.
Vitamin C is essential for collagen synthesis (as the cofactor for prolyl hydroxylase and lysyl hydroxylase — the enzymes that hydroxylate proline and lysine residues in collagen, providing its structural stability). Adequate Vitamin C intake supports the collagen component of articular cartilage matrix. The Framingham Osteoarthritis Cohort Study found that higher dietary Vitamin C intake was associated with a 3-fold reduction in the risk of knee osteoarthritis progression — making Vitamin C one of the few nutrients with prospective cohort evidence for modifying osteoarthritis progression rather than merely reducing symptoms.
3. Turmeric (Curcumin) — The Most Evidence-Backed Natural Joint Remedy
Curcumin — the primary bioactive compound in turmeric — has the most extensive evidence base of any natural compound for osteoarthritis management. Its specific mechanisms are directly relevant to osteoarthritis pathophysiology: curcumin inhibits NF-κB (the master transcription factor for inflammatory gene expression), directly suppressing the production of IL-1β, TNF-α, cyclooxygenase-2 (COX-2), and matrix metalloproteinases (MMPs) that degrade cartilage matrix. It also inhibits the NLRP3 inflammasome — the molecular platform that drives the synovial inflammation of osteoarthritis — and reduces the inducible nitric oxide synthase (iNOS) activity that produces the nitric oxide responsible for chondrocyte apoptosis in osteoarthritic cartilage.
A systematic review and meta-analysis published in the Journal of Medicinal Food covering multiple randomised controlled trials found curcumin supplementation significantly reduced osteoarthritis pain and improved function compared to placebo — with effect sizes comparable to NSAIDs (non-steroidal anti-inflammatory drugs) like ibuprofen, but without the gastrointestinal, renal, and cardiovascular side effects that limit NSAID use in the elderly patients most commonly affected by osteoarthritis. The critical bioavailability requirement — combining curcumin with piperine (black pepper) and a fat source — must be addressed for meaningful therapeutic concentrations to be achieved. The traditional Indian haldi doodh (golden milk) with ghee and black pepper is the optimal bioavailability-enhanced preparation, as covered in our anti-inflammatory foods guide.
4. Ginger — Anti-Inflammatory and Analgesic Properties
Ginger’s gingerols and shogaols inhibit both COX-1 and COX-2 enzymes (the prostaglandin synthesis pathway targeted by NSAIDs) and additionally inhibit 5-lipoxygenase (5-LOX — the leukotriene synthesis pathway) — a dual anti-inflammatory mechanism that NSAIDs do not provide. This dual COX/LOX inhibition is the same mechanism through which some more advanced anti-inflammatory drugs work, but achieved through a natural compound with a significantly superior safety profile for long-term use.
A randomised crossover trial published in Arthritis and Rheumatism found that ginger extract (255mg twice daily) significantly reduced knee pain on standing and pain after walking compared to placebo in knee osteoarthritis patients — with effects maintained at 6-week follow-up and superior tolerability compared to ibuprofen in the same study. A systematic review of ginger for osteoarthritis confirmed significant reductions in pain and disability scores across multiple trials, with no serious adverse effects reported.
Practical applications: Fresh ginger tea (1-inch ginger steeped in boiling water), ginger incorporated generously into daily cooking, and ginger compress applied topically to affected joints (fresh grated ginger in a thin cloth applied warm for 20 minutes) — all deliver therapeutic gingerol concentrations through different routes simultaneously.
5. Boswellia (Shallaki) — The Ayurvedic Resin With Clinical Trial Evidence
Boswellia serrata — known as Shallaki in Ayurveda and commonly sold as “Indian frankincense” — contains boswellic acids (particularly AKBA — 3-O-acetyl-11-keto-β-boswellic acid) that selectively inhibit 5-lipoxygenase (5-LOX) without significantly inhibiting COX enzymes. This selective 5-LOX inhibition reduces leukotriene B4 production — the primary mediator of inflammatory cell chemotaxis into the synovial space — producing anti-inflammatory effects without the COX-inhibition-associated gastrointestinal side effects of conventional NSAIDs.
Multiple randomised controlled trials have documented Boswellia serrata extract’s efficacy for knee osteoarthritis — with a Cochrane-quality systematic review finding significant improvements in pain, stiffness, and physical function compared to placebo. A notable trial published in Phytomedicine found a standardised Boswellia extract produced significant pain reduction within as early as 7 days — faster than most other natural anti-inflammatory agents. Boswellia also specifically inhibits human leukocyte elastase (HLE) — an enzyme that degrades proteoglycans in articular cartilage, suggesting a direct cartilage-protective mechanism beyond simple anti-inflammatory activity.
6. Ashwagandha (Withania somnifera) — Adaptogenic Anti-Inflammatory Joint Support
Ashwagandha’s withanolides have documented anti-inflammatory activity through NF-κB inhibition — the same pathway as curcumin but through different molecular targets, providing complementary anti-inflammatory coverage. Research shows ashwagandha reduces synovial inflammation, reduces inflammatory cytokine production in joint tissue, and improves the systemic inflammatory state that feeds joint disease. A randomised controlled trial on knee osteoarthritis specifically found ashwagandha extract significantly improved pain scores and functional capacity compared to placebo over 12 weeks.
Ashwagandha’s adaptogenic effects — reducing cortisol and HPA axis reactivity — are additionally relevant because chronic stress and cortisol elevation worsen osteoarthritis through increased systemic inflammation, impaired collagen synthesis, and reduced cartilage proteoglycan maintenance. The comprehensive evidence for ashwagandha is in our article on ashwagandha for stress and anxiety.
7. Heat and Cold Therapy — Targeted Symptomatic Relief
Heat and cold applications are among the simplest and most immediately effective osteoarthritis home remedies — with the choice between them dependent on the specific phase of symptoms and the individual’s response.
Heat therapy (warm water soak, warm compress, hot water bottle, heating pad) is most appropriate for chronic osteoarthritis stiffness — particularly morning stiffness and stiffness after periods of inactivity. Heat increases local blood flow, reduces muscle spasm in the periarticular muscles that contribute significantly to osteoarthritis pain, improves tissue extensibility (making subsequent exercise or movement less painful), and activates TRPV1 (heat receptor) pathways that modulate pain signalling in joint afferents. A warm bath or shower before morning exercise or movement significantly reduces the pain of the first movements and improves exercise tolerance.
Cold therapy (ice pack wrapped in cloth, cold compress) is most appropriate for acute flares — periods of increased swelling, warmth, and pain in the joint that indicate an acute synovial inflammatory episode. Cold reduces blood flow and fluid accumulation in the joint space, reduces inflammatory mediator release from the inflamed synovium, and activates TRPM8 (cold receptor) pathways that compete with pain signals through the gate control mechanism. Cold therapy should be applied for 15–20 minutes, not directly against skin (risk of ice burn), and should be followed by rest — not exercise, which would be inappropriate during an acute inflammatory flare.
8. Sesame Oil Massage (Abhyanga) — Ayurvedic Joint Nourishment
The Ayurvedic practice of Abhyanga — warm sesame oil massage — is specifically prescribed in classical Ayurvedic texts for Sandhivata (osteoarthritis) as a Vata-pacifying intervention that both nourishes joint tissue through transdermal delivery of oleic acid and linoleic acid (which have anti-inflammatory properties), and provides the mechanical benefits of massage on periarticular muscle tension, lymphatic drainage, and synovial fluid distribution.
Modern research on topical sesame oil has found that its sesamol content has direct anti-inflammatory and antioxidant activity at the cellular level, and that topical application provides measurable transdermal delivery of sesame oil constituents to deep tissues. A clinical study on knee osteoarthritis specifically found that topical sesame oil application significantly reduced pain and improved functional scores compared to diclofenac gel (a commonly used topical NSAID) — providing remarkable evidence for the clinical equivalence of this traditional Ayurvedic practice to pharmaceutical topical treatment.
Warm sesame oil gently massaged around the affected joint for 10–15 minutes daily (morning is optimal — warming the joint before the day’s activities) reduces stiffness and provides genuine anti-inflammatory support through the sesame oil’s bioactive compounds reaching periarticular tissues.
9. Epsom Salt (Magnesium Sulphate) Soaks — Magnesium for Joint and Muscle Support
Epsom salt soaks — bathing or soaking the affected joint in warm water with dissolved Epsom salt (magnesium sulphate) — provide magnesium through both transdermal absorption and the warm soak’s direct joint comfort benefits. Magnesium is required for over 300 enzymatic reactions including those governing muscle relaxation, nerve function, and the ATP-dependent processes of cartilage matrix synthesis. Magnesium deficiency — prevalent in the Indian urban population — contributes to the muscle cramps and spasms that amplify osteoarthritic joint pain through periarticular muscle dysfunction.
The warm water component of Epsom salt soaks provides the heat therapy benefits described above — particularly valuable for morning stiffness. Dissolving 2–3 tablespoons of Epsom salt per litre of warm water creates a foot, hand, or joint soak of appropriate magnesium concentration. 20 minutes of soaking 2–3 times weekly provides both the thermal benefit and magnesium supplementation that support joint and muscle function in osteoarthritis. The broader role of magnesium in metabolic health is covered in our blood sugar guide.
10. Vitamin D Optimisation — The Joint Health Deficiency Most Indians Have
Vitamin D deficiency — affecting 50–94% of the Indian urban population as covered in our immune system guide — has direct relevance to osteoarthritis beyond its well-known role in calcium absorption and bone health. Vitamin D receptors are expressed on chondrocytes, and Vitamin D signalling regulates multiple aspects of cartilage metabolism: it promotes chondrocyte differentiation, regulates proteoglycan synthesis, and inhibits the MMP-13 (collagenase-3) that degrades type II collagen in articular cartilage. Low Vitamin D levels are associated with more rapid osteoarthritis progression in multiple prospective cohort studies.
Additionally, Vitamin D deficiency produces a specific musculoskeletal syndrome — proximal muscle weakness, bone pain, and fatigue — that can significantly worsen the functional impairment of osteoarthritis and impair the ability to perform therapeutic exercise. Correcting Vitamin D deficiency therefore both addresses a direct cartilage metabolic deficiency and improves the functional capacity that makes exercise-based management possible. 20–30 minutes of morning sunlight and supplementation where deficiency is confirmed are the most accessible interventions.
11. Glucosamine and Chondroitin — The Nuanced Evidence Picture
Glucosamine sulphate and chondroitin sulphate are the most widely used nutritional supplements for osteoarthritis globally — and their evidence base is more nuanced than either their enthusiastic proponents or their skeptical critics suggest.
The most definitive large-scale trial — GAIT (Glucosamine/Chondroitin Arthritis Intervention Trial, funded by the NIH) — found that the combination of glucosamine and chondroitin sulphate significantly reduced pain in the subgroup of participants with moderate-to-severe knee pain (though not in those with mild pain), with an effect size comparable to celecoxib (a prescription NSAID) in this subgroup. Subsequent European trials found crystalline glucosamine sulphate (not hydrochloride) significantly reduced joint space narrowing compared to placebo over 3 years — providing the first structural evidence for a disease-modifying effect of a natural supplement on osteoarthritis progression.
The ESCEO (European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis) guidelines recommend prescription-strength glucosamine sulphate as a first-line symptomatic slow-acting drug for knee osteoarthritis — one of the few natural supplements to achieve this level of clinical guideline endorsement. The current evidence supports use in moderate-to-severe osteoarthritis for a defined trial period (3–6 months) to assess individual response, with continuation only in responders.
12. Stress Management and Sleep — The Systemic Inflammation Connection
Chronic stress and poor sleep both worsen osteoarthritis through systemic inflammatory pathways that directly accelerate cartilage catabolism. Cortisol from chronic HPA axis activation increases the production of inflammatory cytokines including IL-6 and CRP — the same cytokines that drive synovial inflammation and MMP production in osteoarthritic joints. Sleep deprivation independently increases systemic inflammatory markers and reduces the growth hormone secretion that supports cartilage matrix repair. The pain-sleep interaction is bidirectional: osteoarthritis pain impairs sleep, and poor sleep lowers pain thresholds (increasing osteoarthritis pain) — creating a reinforcing cycle that requires active intervention on both fronts.
The yoga and mindfulness approaches most relevant to osteoarthritis management — combining gentle joint movement with the parasympathetic nervous system activation that reduces inflammatory signalling — are covered in our yoga for stress relief guide. The comprehensive sleep optimisation framework connecting sleep quality to systemic inflammatory outcomes is in our healthy morning routine guide.
The Exercise Programme for Osteoarthritis — The Most Important Treatment Available
Exercise is the single most evidence-backed intervention for osteoarthritis — with a 2013 Cochrane review of 54 randomised controlled trials confirming that land-based exercise significantly reduces pain and improves physical function in knee osteoarthritis, with effect sizes comparable to NSAIDs but without their adverse effects. The common fear that exercise “wears out” already damaged joints is not supported by evidence — appropriate exercise actually supports cartilage health by providing the mechanical loading that drives synovial fluid circulation (cartilage is avascular and depends on joint movement for nutrient delivery), and builds the periarticular muscle strength that reduces peak joint contact stress.
The exercise programme should combine three components:
Aerobic Exercise — Low-Impact Joint-Friendly Options
Aerobic exercise improves cardiovascular fitness, supports weight management, reduces systemic inflammation, and improves mood and pain tolerance — all relevant to osteoarthritis management. Low-impact options are preferred to minimise joint contact stress while maintaining aerobic benefit.
Swimming and water aerobics: The buoyancy of water offloads approximately 90% of body weight from lower limb joints while providing resistance for muscle strengthening and cardiovascular conditioning. Research consistently shows water-based exercise produces pain reduction and functional improvement equivalent to land-based exercise with significantly less joint discomfort — making it the ideal starting option for people with significant pain that limits land-based activity.
Cycling (stationary or outdoor): Cycling provides excellent aerobic conditioning with minimal knee joint impact (the load is primarily muscular rather than compressive). A stationary cycle allows resistance and pace adjustment to match current pain and fitness levels. Research shows cycling programmes produce significant knee osteoarthritis symptom improvement over 12 weeks of consistent practice.
Walking: Brisk walking on flat, even surfaces is appropriate for most people with Grades 1–3 knee osteoarthritis and produces both aerobic and weight management benefits relevant to joint health. Walking on rough terrain, up steep hills, or carrying heavy loads is more appropriate for advanced fitness levels. Start with 15–20 minutes daily and build progressively over weeks.
Strengthening Exercises — The Most Important Component
Strengthening the muscles that support and control joint mechanics — particularly the quadriceps for the knee — is the most clinically important exercise component for osteoarthritis. Quadriceps weakness is both a consequence and an accelerating factor of knee osteoarthritis: weak quadriceps produce higher peak knee joint loading (the muscle cannot adequately control the rate of joint loading during movement), impaired proprioception (the quadriceps provide much of the sensory feedback for knee joint position sense), and reduced ambulatory capacity. A 2006 study found quadriceps weakness was a stronger predictor of knee osteoarthritis progression than radiological disease severity at baseline.
Seated leg press: Starting from a comfortable range (not forcing full flexion if painful), the leg press builds quadriceps and gluteal strength with controlled joint loading. 3 sets of 10–15 repetitions at a resistance that allows completion without pain is the appropriate starting point.
Straight leg raise: Lying on the back with one knee bent (foot flat) and one leg straight, lifting the straight leg to 45 degrees and holding for 3 seconds before lowering. This activates the quadriceps without knee joint loading — making it ideal for initial strengthening when any knee flexion is painful. Progress to more loaded exercises as strength develops.
Short arc quads: A towel roll placed under the knee to maintain partial flexion — extending the lower leg through the final 30 degrees of extension. This range activates VMO (vastus medialis oblique — the inner quadriceps muscle critical for patellar tracking and knee stability) with minimal intra-articular pressure.
Mini squats (partial range): Standing with feet shoulder-width apart, lowering into a partial squat (30–45 degrees of knee flexion — not a deep squat). Holding a chair or wall for balance if needed. This builds functional quadriceps and gluteal strength in the range most used in daily activities (standing from a chair, climbing stairs) and produces significantly better functional outcomes than non-functional isolated quadriceps exercises alone.
Hip abductor and external rotator strengthening: Weakness in the hip abductor (gluteus medius) and external rotator muscles produces increased knee valgus (inward collapse) during weight-bearing activities — dramatically increasing medial compartment knee joint stress. Side-lying hip abduction, clamshell exercises, and resistance band hip strengthening are among the most important exercises for patellofemoral and medial compartment knee osteoarthritis.
Flexibility and Range of Motion — Preventing Contracture
Hamstring stretch: Lying on the back, loop a towel or resistance band around one foot. Straighten the leg as fully as comfortable, holding the stretch at the point of tension (not pain) for 30 seconds. Repeat 3 times each leg. Hamstring tightness increases posterior knee forces and impairs quadriceps mechanical advantage — maintaining hamstring flexibility is important for overall knee mechanics.
Calf stretch: Standing facing a wall with one foot forward and one foot back. Keeping the back heel flat on the floor and the back knee straight, lean forward until a stretch is felt in the back calf. Hold 30 seconds. Calf tightness increases Achilles tendon loading and ankle restriction that alter walking mechanics and increase knee stress proximally.
Yoga for joint mobility: Specific yoga poses — particularly Virabhadrasana I (Warrior I) for hip flexor and quadriceps flexibility, Balasana (Child’s Pose) for hip and knee mobility, and Trikonasana (Triangle Pose) for hip and knee alignment — provide both the flexibility and gentle strengthening benefits of a complete practice when adapted to individual limitation. The yoga guidance in our yoga for stress relief guide provides the foundational framework applicable to arthritic management.
The Ayurvedic Framework for Osteoarthritis — Sandhivata
Ayurveda classifies osteoarthritis as Sandhivata — a Vata-predominant disorder of the joints (Sandhi = joint, Vata = the dosha of air and movement, governing all movement and degeneration in the body). The Vata-dominant character of Sandhivata reflects both the typical presentation (dry, crackling, cracking joints; stiffness worse in the morning and in cold/dry weather; pain that is aggravated by cold and relieved by warmth) and the pathophysiology (Vata derangement depletes the Sleshaka Kapha — the joint lubricating fluid equivalent to synovial fluid in Ayurvedic anatomy — leading to dryness, friction, and degeneration of joint structures).
The Ayurvedic treatment framework for Sandhivata is multi-dimensional and remarkably well-aligned with modern rheumatology principles:
Snehana (oleation therapy): Internal and external application of medicated oils — including Mahanarayan Taila (a classical formulation containing sesame oil with numerous anti-inflammatory herbs) and Ksheerabala Taila for internal use — to pacify Vata and replenish joint lubrication. The clinical rationale maps directly onto the modern understanding of omega-3 fatty acids and oleic acid supporting synovial fluid viscosity and anti-inflammatory membrane phospholipid composition.
Swedana (sudation/fomentation therapy): Application of heat through steam, warm herbal poultices (Pinda Sweda — bolus massage with warm rice or herbal preparations wrapped in cloth), or warm medicated oil bathing — producing the vasodilatory, muscle-relaxing, and synovial fluid-promoting effects that modern evidence attributes to heat therapy for arthritis.
Panchakarma procedures: Janu Basti — a specific Ayurvedic procedure in which warm medicated oil is retained over the knee joint for 30–45 minutes within a ring of flour dough — provides sustained deep heat therapy and transdermal delivery of medicinal oil constituents directly to the intra-articular environment. Research on Janu Basti for knee osteoarthritis shows significant reductions in pain scores and improvements in functional capacity, with effects comparable to conventional physiotherapy in some studies.
Rasayana herbs for Sandhivata: Guggul (particularly Yogaraj Guggul formulation), Sallaki (Boswellia), Ashwagandha, Bala (Sida cordifolia), and Guduchi (Tinospora cordifolia) are the primary Ayurvedic anti-inflammatory and joint-nourishing herbs for Sandhivata — several of which (Boswellia, Ashwagandha, Guggul) have independent clinical trial evidence for osteoarthritis efficacy as reviewed above.
Osteoarthritis: Myth vs. Fact
| ❌ The Myth | ✅ The Truth |
|---|---|
| Osteoarthritis is an inevitable consequence of ageing that cannot be influenced | While age is a risk factor for osteoarthritis, it is not a sufficient cause. Multiple modifiable factors — body weight, physical activity level, dietary inflammation, micronutrient status, and mechanical joint use patterns — have profound influences on osteoarthritis development and progression. Lifestyle interventions can significantly slow progression, reduce pain, and preserve function over decades. Age-related risk does not mean age-determined inevitability. |
| Exercise wears out already damaged joints and should be avoided | This is one of the most harmful beliefs in osteoarthritis management. Appropriate exercise is the single most evidence-backed treatment for osteoarthritis and produces outcomes comparable to NSAIDs with zero adverse effects per Cochrane review. Inactivity causes muscle atrophy that increases peak joint loading, reduces cartilage nutrition (which depends on joint movement for synovial fluid circulation), promotes weight gain, and worsens depression and pain tolerance. The knee cartilage of active individuals is generally healthier than that of sedentary individuals at equivalent ages. |
| Glucosamine supplements can regrow damaged cartilage | No supplement, natural or pharmaceutical, can regrow lost articular cartilage. Glucosamine sulphate may slow cartilage loss and provide symptomatic relief in a proportion of patients — this is clinically meaningful but quite different from cartilage regeneration. The realistic expectation is symptom improvement and potentially reduced progression rate — not reversal of established joint damage. |
| Joint replacement is the only effective treatment for severe osteoarthritis | Joint replacement (total knee or hip arthroplasty) produces excellent outcomes for severe Grade IV osteoarthritis with significant functional limitation despite comprehensive non-surgical management. However, the decision for surgery should follow failure of adequate non-surgical management — which includes weight loss, supervised exercise, physiotherapy, pain management, and appropriate injections. Many patients with radiologically severe osteoarthritis have significantly less functional impairment than the X-ray suggests, and function well without surgery on comprehensive conservative management. |
| Osteoarthritis only affects the elderly | While osteoarthritis prevalence increases with age, it is not exclusively an elderly condition. Post-traumatic osteoarthritis (following joint injury — torn ACL, meniscal injury, fracture) can develop in young and middle-aged adults. Metabolic risk factors (obesity, diabetes) lower the age of osteoarthritis onset significantly. In India, floor-sitting work habits and biomechanical factors produce osteoarthritis in women in their 40s at rates substantially higher than age-matched Western populations. |
| NSAIDs are the best long-term treatment for osteoarthritis pain | NSAIDs are highly effective for acute pain management in osteoarthritis — but their long-term use in the elderly is associated with significant gastrointestinal (peptic ulcer, gastrointestinal bleeding), renal (chronic kidney disease progression), and cardiovascular (increased MI and stroke risk) adverse effects that often outweigh their benefits when used chronically. The appropriate role of NSAIDs is for acute flares and short courses — with exercise, weight management, and natural anti-inflammatory strategies providing the safest long-term management framework. |
Related Articles From HerbeeLife
📖 Anti-Inflammatory Foods: 12 Powerful Choices That Fight Disease From the Inside Out
📖 Benefits of Regular Exercise: 10 Powerful Reasons It Transforms Your Longevity
📖 Ashwagandha for Stress and Anxiety: What Actually Happens in Your Body
📖 Yoga for Stress Relief: 12 Powerful Poses and Science-Backed Tips for Beginners
📖 Role of Hydration: 10 Powerful Science-Backed Reasons Water Is Your Best Health Tool
📖 Natural Ways to Boost Your Immune System: 12 Science-Backed Strategies
📖 Weight Loss Diet vs Exercise: The Honest Truth That Finally Settles the Debate
Frequently Asked Questions: Osteoarthritis Home Remedies and Management
Can osteoarthritis be stopped or reversed naturally?
Established cartilage damage from osteoarthritis cannot be reversed — once articular cartilage is lost, it does not regenerate significantly because cartilage is avascular and has very limited regenerative capacity. However, the term “stopping” osteoarthritis is meaningful: consistent lifestyle management (weight loss, regular exercise, anti-inflammatory diet, optimal micronutrient status) can significantly slow disease progression, reduce symptoms to near-normal levels in mild-moderate disease, and preserve joint function for decades. The goal is not cure but effective long-term management — which is entirely achievable for most people with Grades 1–3 osteoarthritis.
What is the single most effective thing I can do for knee osteoarthritis?
If you are overweight or obese, weight loss is the most powerful single intervention — reducing knee joint loading by 3–6kg per kilogram of body weight lost, addressing the metabolic inflammatory burden simultaneously, and producing outcomes comparable to intra-articular steroid injections at 10% body weight loss. If you are at healthy weight, a consistently followed exercise programme (particularly quadriceps and hip strengthening combined with low-impact aerobic exercise) produces the greatest functional improvement and pain reduction. These two interventions — weight management and exercise — have the largest evidence bases and the best long-term outcomes of all osteoarthritis management strategies.
Is turmeric milk (haldi doodh) actually effective for osteoarthritis?
Curcumin — the primary bioactive compound in turmeric — has genuine clinical trial evidence for osteoarthritis pain reduction, with meta-analysis finding effect sizes comparable to NSAIDs. The critical requirement is bioavailability: curcumin is poorly absorbed from plain turmeric in water. The traditional haldi doodh prepared with warm milk (fat source), a pinch of black pepper (piperine increases curcumin absorption by up to 2,000%), and a small amount of ghee provides the bioavailability-optimised preparation that delivers therapeutic curcumin concentrations. Drinking plain turmeric water produces negligible therapeutic curcumin absorption regardless of the quantity used.
How does Boswellia (Shallaki) compare to conventional medications for osteoarthritis?
Multiple randomised controlled trials have compared Boswellia serrata extracts to NSAIDs and celecoxib for knee osteoarthritis. The consensus finding is that Boswellia produces pain reduction comparable to low-to-moderate dose NSAIDs over 8–12 weeks of use, with significantly better gastrointestinal tolerability and without the renal or cardiovascular adverse effects associated with long-term NSAID use. Boswellia is therefore particularly valuable for people who need ongoing anti-inflammatory support but cannot tolerate or should not use NSAIDs long-term — including elderly patients with renal impairment or cardiovascular disease.
What type of exercise is best to avoid for osteoarthritis?
High-impact repetitive joint loading should be minimised in moderate-severe osteoarthritis: running on hard surfaces produces knee joint impact forces 3–4 times body weight per step; heavy contact sports, deep squatting under load, and activities requiring prolonged kneeling on hard surfaces all generate joint contact stresses that may accelerate cartilage loss in already-compromised joints. This does not mean no exercise — it means smart exercise choice: pool swimming, cycling, walking on level surfaces, and guided resistance training within comfortable ranges produce all the benefits of exercise without the joint-damaging peak loads of high-impact activities.
Sources and References
1. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet, 2019.
2. Messier SP et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: the IDEA randomized clinical trial. JAMA, 2013.
3. Bannuru RR et al. Efficacy of curcumin and Boswellia for knee osteoarthritis: systematic review and meta-analysis. Seminars in Arthritis and Rheumatism, 2015.
4. Altman RD, Marcussen KC. Effects of a ginger extract on knee pain in patients with osteoarthritis. Arthritis and Rheumatism, 2001.
5. Fransen M et al. Exercise for osteoarthritis of the knee: a Cochrane systematic review. British Journal of Sports Medicine, 2015.
6. Reginster JY et al. Long-term effects of glucosamine sulphate on osteoarthritis progression. Lancet, 2001.
7. Christensen R et al. Effect of weight reduction in obese patients diagnosed with knee osteoarthritis. Annals of the Rheumatic Diseases, 2007.
Follow HerbeeLife
🌿 Stay connected for more evidence-based joint health, Ayurvedic wisdom, and natural wellness content:
📸 Instagram | 📌 Pinterest | 👥 Facebook | 🐦 X (Twitter)
Final Thoughts: Managing Osteoarthritis Is a Long-Term Practice, Not a Short-Term Treatment
Osteoarthritis does not have a cure — but it has a management framework that, consistently applied, produces outcomes better than most people diagnosed with the condition ever achieve. The difference between someone who is significantly limited at 65 with Grade 3 knee osteoarthritis and someone who functions well with the same radiological severity is not genetics or luck. It is weight management, a consistent exercise habit, an anti-inflammatory dietary pattern, appropriate supplementation, and the consistent application of the natural and Ayurvedic strategies this guide covers.
These are not passive interventions. They require daily consistency. But they are also free, accessible, side-effect-free, and supported by the strongest evidence base of any interventions available for osteoarthritis management. The pharmaceutical industry cannot offer equivalent outcomes with equivalent safety profiles. The evidence says: move your body, manage your weight, reduce inflammation through food, and apply the wisdom that Ayurveda has been encoding in sesame oil and Shallaki for millennia.
Your joints have more capacity to remain functional than the word “degeneration” suggests. Give them what they need to demonstrate it.
⚠️ Medical Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. Osteoarthritis requires diagnosis and management by a qualified physician or rheumatologist. Always consult a healthcare professional before beginning any new exercise programme, particularly if you have significant joint limitation or comorbid conditions. Read full disclaimer →
💬 Which of these osteoarthritis home remedies has made the most difference for you — and have you tried the Boswellia (Shallaki) or Janu Basti approach? Share your experience in the comments. For a condition affecting so many people, real-world experience from those managing it daily is invaluable guidance for others.

