Hemorrhoids — known as piles in common Indian usage and as Arsha in Ayurvedic medicine — are among the most prevalent conditions in the world, affecting approximately 75% of people at some point in their lives and representing one of the most common reasons for colorectal consultations globally. In India specifically, the combination of dietary patterns that have shifted away from fibre-rich traditional foods, prolonged sitting (increasingly common with desk-based work), insufficient physical activity, and limited awareness of early management options has made symptomatic haemorrhoidal disease a significant and growing public health burden.
Despite this prevalence, haemorrhoids remain among the most under-discussed health conditions — the associated embarrassment means many people delay seeking help, manage with inadequate over-the-counter preparations, and allow a condition that is highly treatable in its early stages to progress to a degree requiring surgical intervention. The goal of this guide is to remove that barrier by providing clear, honest, comprehensive information: what haemorrhoids are, what causes them, how the staging system determines appropriate treatment, what natural and Ayurvedic strategies genuinely offer, and when LASER haemorrhoidectomy and other procedural interventions are the right choice.
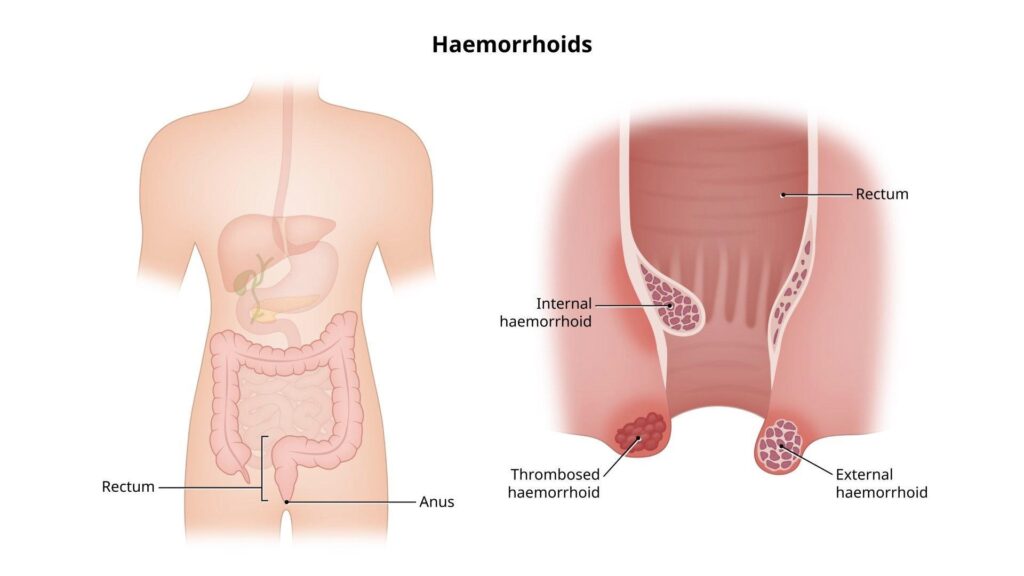
What Haemorrhoids Actually Are — The Anatomy and Physiology
Haemorrhoids are not simply “swollen veins” — a common but incomplete description. They are vascular cushions — specialised anatomical structures composed of submucosal arteriovenous communications, smooth muscle, and connective tissue — that are a normal part of anorectal anatomy present in everyone from birth. Their physiological function is to contribute to fine continence control, supplementing the function of the anal sphincter by creating a compliant, vascular cushion that helps seal the anal canal and sense the difference between gas and stool.
Pathological haemorrhoidal disease occurs when these normal vascular cushions become enlarged, displaced downward from their normal anatomical position, or symptomatic due to mucosal disruption, thrombosis, or prolapse. This distinction — between the normal haemorrhoidal tissue that everyone has and the symptomatic haemorrhoidal disease that requires treatment — is clinically important: the goal of treatment is not to eliminate haemorrhoidal tissue entirely (which would impair continence) but to restore normal anatomy and function by reducing the abnormal enlargement and displacement.

The primary drivers of pathological haemorrhoidal disease are conditions that increase venous pressure in the haemorrhoidal plexus and displace the cushions from their anatomical position: straining during defaecation (the most important and most modifiable single factor), chronic constipation or diarrhoea, prolonged sitting on the toilet (which removes the gravitational support for the anal cushions and increases venous stasis), pregnancy (which increases pelvic venous pressure and compresses the inferior vena cava), chronic cough, obesity, and sedentary lifestyle.
Internal vs. External Haemorrhoids — The Clinical Distinction
Haemorrhoids are anatomically classified by their location relative to the dentate line — the mucocutaneous junction in the anal canal that marks the transition between rectal mucosa (above) and anal skin (below).
Internal haemorrhoids develop above the dentate line, within the rectum. They are covered by rectal mucosa — which contains autonomic (visceral) nerve fibres rather than somatic sensory fibres — meaning they are typically painless unless they prolapse through the anal canal and undergo strangulation. The most common symptom of internal haemorrhoids is bright red rectal bleeding during defaecation — typically described as blood on the tissue paper or dripping into the toilet bowl, separate from the stool rather than mixed with it. This distinction from blood mixed with stool (which raises concern for a higher colorectal source) is clinically important and should always be assessed by a physician.
External haemorrhoids develop below the dentate line, covered by anal skin that contains somatic sensory nerve fibres — making them exquisitely sensitive to pain, particularly when thrombosis (clotting) occurs within the haemorrhoidal tissue. An acutely thrombosed external haemorrhoid presents as a sudden-onset, very painful, firm lump at the anal margin — often following a specific precipitant (straining, heavy lifting, long car journey). This acute presentation is one of the most painful anorectal conditions and often prompts urgent medical attention.
Mixed haemorrhoids have both internal and external components that meet at the dentate line — the most common clinical presentation in patients with advanced haemorrhoidal disease.
Grading Internal Haemorrhoids — The System That Determines Treatment
Internal haemorrhoids are classified by a four-grade system that directly determines the appropriate management approach — from conservative lifestyle modification to procedural intervention:
Grade I: Haemorrhoids that bleed during defaecation but do not prolapse below the dentate line. Only visible on anoscopy. Managed effectively with dietary modification, fibre supplementation, adequate hydration, straining avoidance, and topical agents. No procedural intervention required in most cases.
Grade II: Haemorrhoids that prolapse through the anus during defaecation but reduce spontaneously (retract back inside without assistance) after the bowel movement. Conservative management is still the first line — with office-based procedures (rubber band ligation, sclerotherapy) as second-line if conservative management fails.
Grade III: Haemorrhoids that prolapse and require manual reduction by the patient (pushing back inside with a finger). Typically symptomatic with prolapse discomfort, mucous discharge, perianal soiling, and sometimes bleeding. Office-based procedures and LASER-based interventions are appropriate at this grade.
Grade IV: Permanently prolapsed haemorrhoids that cannot be reduced manually, or acutely thrombosed/strangulated haemorrhoids. This grade requires surgical intervention — haemorrhoidectomy (LASER, stapled, or conventional) is the appropriate treatment.
This grading framework is the key clinical insight for understanding when different treatment levels are appropriate. Grades I and II are primarily a dietary and lifestyle problem addressable with natural interventions. Grade III benefits from both lifestyle optimisation and procedural treatment. Grade IV requires surgery. Applying Grade IV surgical treatments to Grade I haemorrhoids (or hoping Grade IV will resolve with dietary fibre alone) are both misalignments of treatment to severity that produce avoidable suffering.
10 Natural Remedies and Lifestyle Strategies for Haemorrhoid Management
For Grade I and II haemorrhoids — and as foundational management for all grades — the natural strategies below represent the most evidence-supported non-surgical approaches available. They address the primary drivers of haemorrhoidal disease at their root rather than merely managing symptoms.
1. Dietary Fibre — The Most Important Single Intervention
Dietary fibre is the most consistently evidence-backed non-pharmacological treatment for haemorrhoidal disease — with multiple randomised controlled trials confirming that fibre supplementation significantly reduces bleeding, prolapse, and the overall symptom score of haemorrhoids independent of other management. A meta-analysis published in the American Journal of Gastroenterology found that dietary fibre supplementation reduced the risk of persistent haemorrhoidal symptoms and bleeding by approximately 50% compared to control conditions.
The mechanism is direct: adequate dietary fibre (25–35g daily from whole food sources) increases stool bulk and softness, reduces colonic transit time, and eliminates the need for straining at defaecation — the single most important mechanical driver of haemorrhoidal enlargement and displacement. Every bowel movement that occurs without straining reduces the vascular pressure in the haemorrhoidal plexus and allows the displaced cushions to gradually return toward their normal anatomical position.
For the Indian diet specifically, the most fibre-rich whole food sources are: psyllium husk (isabgol) — the most used and most evidence-backed fibre supplement globally, with 5–10g per dose providing 70–80% soluble fibre that forms a gel reducing straining; dal and legumes (all varieties — the most bioavailable plant fibre sources in Indian cooking); whole grains including millets (ragi, bajra, jowar provide significantly more fibre than refined wheat or white rice); seasonal vegetables; and fresh fruits with skin intact. The comprehensive dietary fibre and gut health strategy is covered in our guide to improving digestion naturally.
2. Adequate Hydration — The Fibre Companion
Fibre’s stool-softening mechanism requires adequate water intake to function — fibre absorbs and retains water to form the bulk and softness that reduces straining. Without adequate hydration, increased fibre intake can paradoxically worsen constipation by creating dry, bulky stool that is harder to pass. The target of 30–35ml per kg of body weight daily — covered in our hydration guide — supports haemorrhoid management directly through stool consistency optimisation.
3. Correct Defaecation Posture and Behaviour — The Squatting Advantage
Defaecation posture is one of the most underappreciated and most modifiable factors in haemorrhoidal disease — and one where traditional Indian toilet practices have a significant anatomical advantage over Western seated toilets. The Western seated toilet position creates an anorectal angle that requires greater straining effort for complete evacuation — the puborectalis muscle maintains partial contraction in the seated position, preserving an anorectal angle that restricts stool passage. The squatting position fully relaxes the puborectalis, straightens the anorectal angle, and allows evacuation with minimal straining effort.
Research published in the Journal of Clinical Gastroenterology confirmed that squatting (using a squatting platform or toilet footstool to elevate the feet while seated) significantly reduced defaecation time, reduced straining effort, and improved the sense of complete evacuation compared to standard seated defaecation. For people using Western toilets, a footstool (such as the widely marketed Squatty Potty) that elevates the feet to hip height replicates the anorectal angle of squatting while maintaining the comfort of a seated toilet. This simple, inexpensive intervention addresses the mechanical driver of haemorrhoidal disease at every defaecation rather than only during treatment sessions.
Behavioural guidance: do not spend more than 3–5 minutes on the toilet; do not use mobile phones, newspapers, or other reading materials on the toilet (which prolongs sitting time and unconsciously increases straining); respond promptly to the defaecatory urge rather than delaying (delayed defaecation allows stool to dry and harden, increasing straining at the next attempt).
4. Sitz Baths — The Most Evidence-Backed Symptomatic Relief
Sitz baths — soaking the perianal area in warm water (not hot) for 10–15 minutes, 2–3 times daily and particularly after bowel movements — are the most consistently recommended and most evidence-supported symptomatic relief measure for all types of haemorrhoidal disease. The warm water reduces external and internal anal sphincter spasm (which contributes significantly to haemorrhoidal pain, particularly with thrombosed haemorrhoids), improves local circulation to support healing, provides gentle hygiene that reduces the irritation from perianal soiling, and produces the vasodilatory effect that reduces haemorrhoidal engorgement.
Research comparing sitz baths to other symptomatic interventions consistently shows them as effective as or superior to topical anaesthetic preparations for pain relief — with the additional benefit of sphincter relaxation that topical agents cannot provide. Plain warm water is adequate — the addition of Epsom salts or other additives provides negligible additional benefit over warm water alone and can occasionally cause skin irritation in sensitive perianal skin.
5. Cold Compress for Acute Thrombosed Haemorrhoids
For acutely thrombosed external haemorrhoids — the extremely painful sudden-onset perianal lump — cold application (wrapped ice pack or cold compress applied to the perianal area for 10–15 minutes several times daily) provides meaningful pain relief through vasoconstriction that reduces the acute swelling and inflammation of the thrombosed tissue. Cold compress is most effective in the first 24–48 hours of thrombosis onset, during which the clot is still fresh and the associated oedema most pronounced. After 48–72 hours, switching to warm sitz baths supports the natural reabsorption of the clot that produces gradual resolution of most thrombosed external haemorrhoids over 1–4 weeks.
6. Witch Hazel — The Topical Astringent With Evidence
Witch hazel (Hamamelis virginiana) extract — available as a liquid astringent at most Indian pharmacies — is one of the most studied topical preparations for haemorrhoidal symptoms, with documented efficacy for reducing bleeding, itching, and discomfort through its tannin content. Tannins produce protein precipitation on the mucosal surface, creating an astringent barrier that reduces haemorrhoidal secretions, moderates bleeding through a mild haemostatic effect, and reduces the perianal irritation that causes itching.
The topical application of witch hazel on a soft cotton pad to the perianal area after bowel movements provides rapid symptom relief for the itching and discomfort of external haemorrhoids and haemorrhoidal prolapse. It is safe for regular use and significantly better tolerated than many commercial haemorrhoidal preparations that contain local anaesthetics (which can cause contact sensitisation with prolonged use).
7. Triphala — Ayurveda’s Best-Evidenced Digestive and Haemorrhoidal Herb
Triphala — the three-fruit Ayurvedic formulation of amla, haritaki, and bibhitaki — is the most important single Ayurvedic preparation for haemorrhoidal disease (Arsha) and one of the few Ayurvedic preparations with direct clinical trial evidence for this indication. Triphala addresses haemorrhoids through multiple mechanisms: haritaki’s documented laxative and colon-motility-enhancing effects reduce constipation and straining; amla’s anti-inflammatory and mucosal-healing properties reduce haemorrhoidal inflammation and support mucosal repair; bibhitaki’s astringent tannins reduce haemorrhoidal secretions and bleeding; and the combined prebiotic effect of all three fruits supports the microbiome diversity that maintains normal bowel regularity.
A randomised controlled trial found Triphala supplementation significantly improved functional constipation and bowel regularity — the primary driver of haemorrhoidal disease — with effects maintained without tolerance development. For haemorrhoidal management specifically, Triphala powder (half to one teaspoon in warm water) before bed is the standard Ayurvedic preparation — taken consistently over weeks to months as a gentle preventive and therapeutic intervention. The full evidence for Triphala is covered in our digestion guide.
8. Aloe Vera — Anti-Inflammatory Topical Soothing
Aloe vera gel applied topically to the perianal area provides the anti-inflammatory, wound-healing, and cooling effects that make it one of the most accessible natural topical agents for haemorrhoidal discomfort. Its acemannan content stimulates macrophage activity and collagen synthesis — supporting the repair of any mucosal disruption associated with prolapsed or bleeding haemorrhoids. Its cooling, demulcent quality provides immediate symptomatic relief for the burning and irritation of perianal inflammation. And its natural antimicrobial properties reduce the bacterial colonisation of any disrupted perianal skin.
For internal haemorrhoids specifically, aloe vera gel can be gently applied internally using a clean finger — a traditional practice in Ayurvedic and folk medicine that provides the anti-inflammatory and healing benefits at the site of the haemorrhoidal tissue itself.
9. The Arsha (Piles) Ayurvedic Framework — Ksharakarma and Agnikarma
Ayurveda has one of the most sophisticated historical frameworks for haemorrhoidal disease — Arsha is classified in classical Ayurvedic texts alongside anal fissure and fistula as conditions of the anorectal region (Gudagata Roga), and the Sushruta Samhita devotes extensive sections to its classification, pathogenesis, and management.
Ayurveda classifies Arsha into two primary types: Sushka Arsha (dry piles — predominantly Vata and Kapha, producing large, solid masses without bleeding) and Rakta Arsha (bleeding piles — predominantly Pitta, with bleeding and inflammation). This distinction maps onto the internal/external and inflammatory/non-inflammatory clinical distinctions of modern proctology.
Ksharakarma — the application of alkaline medicinal preparations to the haemorrhoidal tissue — is the classical Ayurvedic procedural treatment for Arsha. Kshara (alkaline herbal preparations, most commonly prepared from Apamarga — Achyranthes aspera) is applied directly to haemorrhoidal tissue under direct vision, causing chemical coagulation and shrinkage of the haemorrhoidal mass. This procedure is described in the Sushruta Samhita with clinical detail that predates modern sclerotherapy by over 2,500 years — and modern research has confirmed that Ksharakarma produces clinical outcomes comparable to rubber band ligation for Grade I and II internal haemorrhoids, with the additional advantage of being a single-session outpatient procedure with minimal post-procedure discomfort. Several Ayurvedic hospitals in India perform Ksharakarma with documented clinical outcomes.
Agnikarma — thermal cauterisation using a specialised metal instrument — is the Ayurvedic equivalent of modern infrared coagulation or laser photocoagulation, and represents another area of remarkable Ayurvedic clinical prescience that predates modern equivalents by millennia.
10. Regular Physical Activity — The Constipation and Venous Stasis Remedy
Physical activity promotes bowel regularity through multiple mechanisms: stimulating colonic motility through autonomic nervous system effects, reducing transit time, reducing the portal venous hypertension that contributes to haemorrhoidal engorgement, and reducing the prolonged sitting that produces the venous stasis driving haemorrhoidal congestion. A sedentary desk-based lifestyle is an independent risk factor for haemorrhoidal disease — and regular daily walking is one of the most accessible and most effective preventive interventions. The comprehensive evidence for exercise and digestive health is covered in our benefits of regular exercise guide.
Medical and Procedural Treatments — When Natural Management Needs Support
Office-Based Procedures — Grade I to III
Rubber band ligation (RBL) is the most widely performed and most evidence-supported office-based procedure for Grade I to III internal haemorrhoids — with clinical trials consistently showing it to be superior to other non-surgical approaches including sclerotherapy and infrared coagulation in terms of symptom resolution and recurrence rates. A rubber band is applied to the base of the haemorrhoidal tissue above the dentate line — the resulting ischaemia causes the haemorrhoidal tissue to necrose and slough over 5–7 days, leaving a small scar that anchors the remaining mucosa in its normal anatomical position. It is performed in the outpatient clinic without anaesthesia (bands are placed above the dentate line, in non-sensate mucosa), with minimal discomfort and a return to normal activities within 24 hours for most patients. Recurrence rates at 2 years are approximately 30–40%, making repeat banding the appropriate response to recurrence rather than surgical escalation.
Sclerotherapy — injection of a sclerosant agent (phenol in oil or quinine urea) into the haemorrhoidal pedicle above the dentate line — produces fibrosis that shrinks the haemorrhoidal tissue and fixes the mucosa to the underlying muscle, preventing further prolapse. It is most effective for Grade I and II bleeding haemorrhoids and is particularly appropriate for patients on anticoagulant therapy (in whom rubber band ligation carries higher bleeding risk) and for elderly patients with multiple comorbidities where more invasive procedures pose disproportionate risk.
LASER Haemorrhoidectomy — The Advanced Surgical Option
LASER haemorrhoidectomy uses focused laser energy — typically from a neodymium-doped yttrium aluminium garnet (Nd:YAG) or diode laser (980nm or 1470nm wavelengths) — to ablate haemorrhoidal tissue through photocoagulation. The laser energy is absorbed by haemoglobin and water in the haemorrhoidal vasculature, converting to heat that coagulates the blood supply to the haemorrhoidal pedicle and causes thermal ablation of the haemorrhoidal mass with simultaneous sealing of the surrounding tissue.
The clinical advantages of LASER haemorrhoidectomy over conventional surgical haemorrhoidectomy (where haemorrhoidal tissue is excised with a scalpel or electrocautery) are well-documented and include: significantly reduced post-operative pain (the precision of laser energy minimises collateral thermal damage to the richly innervated perianal skin and muscle), reduced intra-operative bleeding (the coagulation effect seals blood vessels as it cuts), faster wound healing (reduced tissue trauma accelerates healing), shorter hospital stay (typically day-case procedure under local or spinal anaesthesia), and earlier return to normal activities (most patients return to work within 1–2 weeks compared to 3–4 weeks for conventional haemorrhoidectomy).
A systematic review comparing LASER haemorrhoidectomy to conventional Milligan-Morgan haemorrhoidectomy found significant advantages for LASER in post-operative pain scores, analgesic requirement, time to return to work, and patient satisfaction — with equivalent or superior haemorrhoid control rates at one-year follow-up. For Grade III and IV haemorrhoids that have not responded to conservative management and office-based procedures, LASER haemorrhoidectomy represents the current best-practice surgical option.
The specific LASER procedures available include: Laser Haemorrhoidoplasty (LHP) — laser coagulation of the haemorrhoidal vascular pedicle without formal excision, most appropriate for Grade II and III; and formal LASER haemorrhoidectomy for Grade III and IV disease, combining laser excision of the haemorrhoidal mass with laser coagulation of the pedicle.
Stapled Haemorrhoidopexy (PPH) — The Procedure for Circumferential Prolapse
Stapled haemorrhoidopexy (Procedure for Prolapse and Haemorrhoids — PPH) uses a circular stapling device to resect a circumferential ring of prolapsed rectal mucosa above the haemorrhoidal tissue, pulling the haemorrhoidal cushions back into their normal anatomical position and interrupting their blood supply simultaneously. It is particularly appropriate for circumferential Grade III prolapse where multiple haemorrhoidal columns have prolapsed together. Its advantage is minimal post-operative pain (the staple line is placed in non-sensate mucosa above the dentate line) — its limitation is a higher recurrence rate than conventional haemorrhoidectomy for Grade IV disease.
Haemorrhoids and Pregnancy — Special Considerations
Haemorrhoidal disease is extremely common during pregnancy — affecting approximately 30–40% of pregnant women, particularly in the third trimester and postpartum period. The combination of increased pelvic venous pressure from the enlarging uterus, constipation (from progesterone-driven reduced gut motility and iron supplementation), and the bearing-down effort of labour creates the ideal conditions for haemorrhoidal development and exacerbation.
Management during pregnancy and breastfeeding is appropriately conservative: dietary fibre and adequate hydration are the primary interventions; sitz baths provide safe symptomatic relief; topical witch hazel and aloe vera are appropriate; and Triphala in moderate doses is generally considered safe (though the laxative effect should be monitored). Most haemorrhoids that develop or worsen during pregnancy improve significantly or resolve completely within weeks to months of delivery — meaning procedural intervention is rarely required during pregnancy itself. Any haemorrhoidal bleeding during pregnancy should be assessed by a physician to exclude other causes of rectal bleeding, which require different management.
Warning Signs — When Rectal Bleeding Is Not Just Haemorrhoids
The most important clinical safety message in any guide to haemorrhoidal disease is this: not all rectal bleeding is from haemorrhoids, and assuming haemorrhoidal aetiology without appropriate assessment risks missing colorectal cancer, inflammatory bowel disease, colonic polyps, and other conditions that require prompt diagnosis and treatment.
Seek medical evaluation for: rectal bleeding in anyone over 40 without a prior confirmed haemorrhoidal diagnosis; bleeding that is dark red or maroon (suggesting a higher colorectal source) rather than bright red; bleeding associated with a change in bowel habit (increased frequency, looser stools, urgency, or the sensation of incomplete evacuation); bleeding accompanied by mucus or pus in the stool; unexplained weight loss alongside rectal bleeding; rectal bleeding in a person with a family history of colorectal cancer or polyposis; any new rectal bleeding that does not clearly have an anatomically explicable haemorrhoidal basis; and any anal mass, lump, or ulcer that has not been professionally evaluated. These presentations require colonoscopy or sigmoidoscopy to exclude significant pathology — they cannot be safely attributed to haemorrhoids on symptom history alone.
Haemorrhoids: Myth vs. Fact
| ❌ The Myth | ✅ The Truth |
|---|---|
| Haemorrhoids always need surgery | The vast majority of haemorrhoidal disease (Grade I and II) resolves completely or becomes asymptomatic with dietary fibre optimisation, adequate hydration, defaecation habit correction, and topical symptomatic management. Surgery (including LASER haemorrhoidectomy) is appropriate only for Grade III and IV disease that has not responded to conservative management and office-based procedures. Most people who seek treatment for haemorrhoids never require surgery. |
| Haemorrhoids only affect elderly people | Haemorrhoidal disease is most prevalent in adults aged 45–65, but occurs across all adult age groups and is increasingly common in younger adults due to sedentary lifestyles, low-fibre diets, and desk-based work. It is also very common in pregnancy and postpartum, affecting up to 40% of pregnant women. |
| Spicy food causes haemorrhoids | Spicy food is a very common aggravating factor that worsens the symptoms of existing haemorrhoids — particularly the burning and irritation — but does not cause haemorrhoidal disease. The primary causes are dietary fibre deficiency, chronic constipation, straining, and prolonged sitting. Temporarily reducing very spicy food during active haemorrhoidal episodes is reasonable for symptom management, but long-term avoidance of spicy food is unnecessary for haemorrhoidal prevention in people with adequate fibre intake and normal defaecation habits. |
| Haemorrhoids are always painful | Internal haemorrhoids — the most common type — are typically painless because they are located above the dentate line in mucosa with only autonomic nerve supply. Many people have significant internal haemorrhoidal disease with Grade II prolapse and bleeding without any pain. Pain is characteristic of external haemorrhoids (particularly acutely thrombosed), prolapsed and strangulated internal haemorrhoids, and conditions that coexist with haemorrhoids (anal fissure, perianal abscess). |
| All rectal bleeding is from haemorrhoids and can be self-managed | Rectal bleeding requires professional medical assessment in all adults who have not had recent colorectal investigation — particularly those over 40, those with any associated change in bowel habit, and those with risk factors for colorectal cancer. Haemorrhoidal bleeding is the most common cause of rectal bleeding, but assuming haemorrhoidal aetiology without assessment risks missing colorectal cancer or other serious conditions. A medical examination takes minutes; missing a treatable cancer can cost years of life. |
| Once you have haemorrhoids, they will always recur after treatment | The recurrence rate after haemorrhoidal treatment depends on whether the causative factors are addressed. Haemorrhoids that are treated procedurally or surgically without addressing the dietary fibre deficiency, constipation, and straining that caused them will recur — because the tissue has been treated but the mechanical stress continues. Haemorrhoids treated in the context of comprehensive lifestyle modification (adequate fibre, hydration, exercise, defaecation habit correction) have significantly lower recurrence rates. Treatment is most durable when it accompanies genuine root-cause management. |
Related Articles From HerbeeLife
📖 How to Improve Digestion Naturally: 12 Powerful Science-Backed Strategies
📖 Anti-Inflammatory Foods: 12 Powerful Choices That Fight Disease From the Inside Out
📖 Role of Hydration: 10 Powerful Science-Backed Reasons Water Is Your Best Health Tool
📖 Benefits of Regular Exercise: 10 Powerful Reasons It Transforms Your Health
📖 Healthy Snacks: 15 Options That Are High in Fibre and Actually Filling
📖 Amla Benefits: Proven Immunity, Digestion and Whole-Body Health
📖 Holistic Health Benefits: 7 Life-Changing Reasons to Treat Your Whole Self
Frequently Asked Questions: Haemorrhoids and LASER Treatment
Can haemorrhoids heal completely on their own?
Grade I and mild Grade II haemorrhoids frequently resolve completely with consistent dietary and lifestyle modifications — particularly when high fibre intake eliminates straining and normal defaecation is restored. Small thrombosed external haemorrhoids typically resolve spontaneously over 1–4 weeks as the clot is reabsorbed. Grade III and IV haemorrhoids do not resolve without procedural or surgical intervention — the mechanical displacement of the tissue is not reversible by dietary measures alone at these grades.
Is LASER haemorrhoidectomy painful?
LASER haemorrhoidectomy is significantly less painful than conventional haemorrhoidectomy — one of its primary documented advantages. The procedure itself is performed under spinal or general anaesthesia, so there is no pain during the procedure. Post-operative pain is substantially less than conventional surgery, with most patients managing with regular paracetamol and anti-inflammatory medication rather than opioid analgesia. Some discomfort with bowel movements in the first week is expected and normal — managed with stool softeners and sitz baths.
How quickly can I return to normal activities after LASER haemorrhoidectomy?
Most patients undergoing LASER haemorrhoidectomy for Grade III haemorrhoids return to office-based work within 5–7 days and to full physical activity within 2–3 weeks. Conventional haemorrhoidectomy typically requires 3–4 weeks recovery. The faster return to activity is one of the most clinically meaningful advantages of LASER over conventional surgery — particularly for working adults in their productive years.
What is the Ayurvedic Ksharakarma treatment for piles and does it work?
Ksharakarma — the Ayurvedic procedure of applying alkaline herbal preparations (Kshara, typically prepared from Apamarga/Achyranthes aspera) directly to haemorrhoidal tissue — is a well-documented and genuinely effective procedure for Grade I and II internal haemorrhoids. Clinical comparisons with rubber band ligation (the standard office procedure for the same grade) have found comparable efficacy for bleeding control and haemorrhoidal size reduction, with the advantage of being a single-session procedure with minimal post-procedure discomfort. It should be performed by qualified Ayurvedic practitioners with appropriate training and equipment — not attempted at home.
How do I prevent haemorrhoids from recurring after treatment?
Long-term recurrence prevention requires sustained attention to the dietary and lifestyle factors that caused the haemorrhoids: maintaining 25–35g of daily dietary fibre from whole food sources (particularly psyllium husk, dal, vegetables, and whole grains); 2–3 litres of fluid daily; regular bowel habits with immediate response to defaecatory urge; defaecation posture correction (footstool to approximate squatting); no more than 3–5 minutes per toilet visit without screen or reading distractions; regular physical activity; and weight management. These are permanent lifestyle commitments rather than temporary remedies — haemorrhoids are the consequence of lifestyle factors that will reproduce the condition if sustained after treatment.
Sources and References
1. Mott T et al. Hemorrhoids: Diagnosis and treatment options. American Family Physician, 2018.
2. Alonso-Coello P et al. Fiber for the treatment of hemorrhoids complications: a systematic review and meta-analysis. American Journal of Gastroenterology, 2006.
3. Bharat S et al. Laser hemorrhoidoplasty vs conventional Milligan-Morgan hemorrhoidectomy. Indian Journal of Surgery, 2019.
4. Gupta PJ. Kshara Karma — an Ayurvedic treatment for hemorrhoids. Journal of Gastrointestinal and Liver Diseases, 2006.
5. Fontem RF, Abkin M. Internal hemorrhoids. StatPearls Publishing, 2023.
6. Sakr MF, Moussa MM. LigaSure hemorrhoidectomy versus conventional diathermy for outpatient treatment of hemorrhoids. Diseases of the Colon and Rectum, 2010.
7. Simillis C et al. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. British Journal of Surgery, 2015.
Follow HerbeeLife
🌿 Stay connected for more evidence-based digestive health, Ayurvedic wisdom, and natural wellness content:
📸 Instagram | 📌 Pinterest | 👥 Facebook | 🐦 X (Twitter)
Final Thoughts: Haemorrhoids Are Preventable and Treatable — But Only If You Don’t Ignore Them
Haemorrhoids carry a social stigma that keeps too many people suffering in silence — managing inadequately at home, delaying professional assessment, and allowing a highly treatable Grade I or II condition to progress to a Grade III or IV requiring surgery. The condition does not deserve this stigma, and the suffering it causes does not need to be endured.
The natural interventions in this guide — dietary fibre, adequate hydration, defaecation posture correction, sitz baths, Triphala, and regular exercise — are not minor comfort measures. They address the fundamental causes of haemorrhoidal disease at their root and produce genuine resolution of early-stage disease when consistently applied. For Grade III and IV disease, LASER haemorrhoidectomy offers a significantly less painful, faster-recovery surgical option than the conventional procedures that previously deterred many people from seeking the surgical help they needed.
The most important thing you can do for haemorrhoidal health today is have adequate fibre at every meal, drink your water, use your defaecation posture correctly, and see a doctor — without embarrassment — if you have persistent rectal bleeding, prolapse, or discomfort that home management has not resolved.
⚠️ Medical Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. Rectal bleeding and anorectal symptoms require professional medical evaluation to exclude serious conditions. Always consult a qualified colorectal surgeon or gastroenterologist for diagnosis and management of haemorrhoids. Read full disclaimer →
💬 Have you found a natural remedy or lifestyle change that made a significant difference to your haemorrhoidal symptoms — or have you undergone LASER haemorrhoidectomy and want to share your experience? This is a topic many people need help with but few speak openly about. Your experience could genuinely help someone else.

